
Longitudinal Trends in Blood Pressure Associated with The Changes in Living Environment Caused by the Great East Japan Earthquake: The Fukushima Health Management Survey
 , , , , , ,
, , , , , ,
Abstract
:1. Introduction
2. Methods
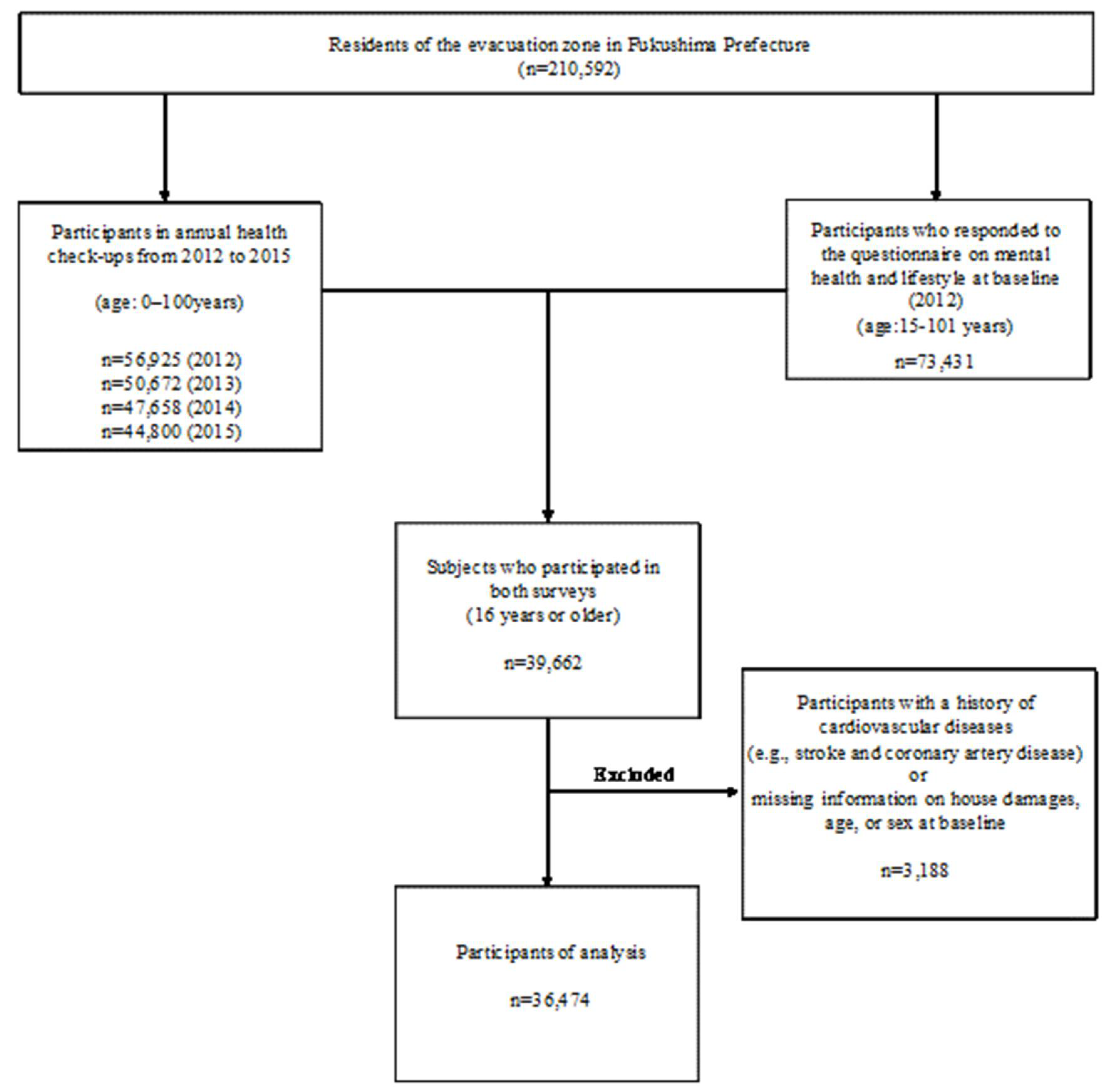
2.1. Study Sample
2.2. Questionnaire Survey on Living Environment Changes
2.3. Blood Pressure Measurement
2.4. Other Covariates
2.5. Ethical Approval
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Koyama, S.; Aida, J.; Kawachi, I.; Kondo, N.; Subramanian, S.V.; Ito, K.; Kobashi, G.; Masuno, K.; Kondo, K.; Osaka, K. Social support improves mental health among the victims relocated to temporary housing following the Great East Japan Earthquake and Tsunami. Tohoku J. Exp. Med. 2014, 234, 241–247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kılıc, C.; Aydın, I.; Taşkıntuna, N.; Özçürümez, G.; Kurt, G.; Eren, E.; Lale, T.; Ozel, S.; Zileli, L. Predictors of psychological distress in survivors of the 1999 earthquakes in Turkey: Effects of relocation after the disaster. Acta Psychiatr. Scand. 2006, 114, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Cao, X.; Jiang, X.; Pang, S.; Li, S.; Cheng, Y.; Tian, L. The prevalence and risk factors for psychological distress in older men and women affected by the Wenchuan, China earthquake. Australas. J. Ageing 2014, 33, E20–E26. [Google Scholar] [CrossRef] [PubMed]
- Nishi, N.; Yoshimura, E.; Ishikawa-Takata, K.; Tsuboyama-Kasaoka, N.; Kubota, T.; Miyachi, M.; Tokudome, S.; Yokoyama, Y.; Sakata, K.; Kobayashi, S.; et al. Relationship of living conditions with dietary patterns among survivors of the great East Japan earthquake. J. Epidemiol. 2013, 23, 376–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohira, T.; Roux, A.V.D.; Prineas, R.J.; Kizilbash, M.A.; Carnethon, M.R.; Folsom, A.R. Associations of psychosocial factors with heart rate and its short-term variability: Multi-ethnic study of atherosclerosis. Psychosom. Med. 2008, 70, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Nishina, M.; Nishina, K.; Ohira, T.; Makino, K.; Iso, H. Associations of psychological distress with metabolic syndrome among Japanese urban residents. J. Atheroscler. Thromb. 2011, 18, 396–402. [Google Scholar] [CrossRef] [Green Version]
- Iso, H.; Date, C.; Yamamoto, A.; Toyoshima, H.; Tanabe, N.; Kikuchi, S.; Kondo, T.; Watanabe, Y.; Wada, Y.; Ishibashi, T.; et al. Perceived mental stress and mortality from cardiovascular disease among Japanese men and women. Circulation 2002, 106, 1229–1236. [Google Scholar] [CrossRef] [Green Version]
- Kivimäki, M.; Virtanen, M.; Elovainio, M.; Kouvonen, A.; Väänänen, A.; Vahtera, J. Work stress in the etiology of coronary heart disease—A meta-analysis. Scand. J. Work. Environ. Health 2006, 32, 431–442. [Google Scholar] [CrossRef]
- Trichopoulos, D.; Katsouyanni, K.; Zavitsanos, X.; Tzonou, A.; Dalla-Vorgia, P. Psychological stress and fatal heart attack: The Athens (1981) earthquake natural experiment. Lancet 1983, 321, 441–444. [Google Scholar] [CrossRef]
- Varghese, T.; Hayek, S.S.; Shekiladze, N.; Schultz, W.M.; Wenger, N.K. Psychosocial Risk Factors Related to Ischemic Heart Disease in Women. Curr. Pharm. Des. 2016, 22, 3853–3870. [Google Scholar] [CrossRef]
- Rosengren, A.; Hawken, S.; Ôunpuu, S.; Sliwa, K.; Zubaid, M.; Almahmeed, W.A.; Blackett, K.N.; Sitthi-amorn, C.; Sato, H.; Yusuf, S. Association of psychosocial risk factors with risk of acute myocardial infarction in 11 119 cases and 13 648 controls from 52 countries (the INTERHEART study): Case-control study. Lancet 2004, 364, 953–962. [Google Scholar] [CrossRef] [PubMed]
- Truelsen, T.; Nielsen, N.; Boysen, G.; Grønbæk, M. Self-reported stress and risk of stroke. Stroke 2003, 34, 856–862. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Everson, S.A.; Lynch, J.W.; Kaplan, G.A.; Lakka, T.A.; Sivenius, J.; Salonen, J.T. Stress-induced blood pressure reactivity and incident stroke in middle-aged men. Stroke 2001, 32, 1263–1270. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Nakano, H.; Nagai, M.; Yumiya, Y.; Zhang, W.; Uemura, M.; Sakai, A.; Hashimoto, S.; for the Fukushima Health Management Survey Group. Changes in Cardiovascular Risk Factors After the Great East Japan Earthquake. Asia Pac. J. Public Health 2017, 29, 47S–55S. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Hosoya, M.; Yasumura, S.; Satoh, H.; Suzuki, H.; Sakai, A.; Ohtsuru, A.; Kawasaki, Y.; Takahashi, A.; Ozasa, K.; et al. Evacuation and Risk of Hypertension After the Great East Japan Earthquake. Hypertension 2016, 68, 558–564. [Google Scholar] [CrossRef]
- Cwikel, J.G.; Goldsmith, J.R.; Kordysh, E.; Quastel, M.; Abdelgani, A. Blood pressure among immigrants to Israel from areas affected by the Chernobyl disaster. Public Health Rev. 1997, 25, 317–335. [Google Scholar]
- Yasumura, S.; Ohira, T.; Ishikawa, T.; Shimura, H.; Sakai, A.; Maeda, M.; Miura, I.; Fujimori, K.; Ohto, H.; Kamiya, K. Achievements and Current Status of the Fukushima Health Management Survey. J. Epidemiol. 2022, 32, S3–S10. [Google Scholar] [CrossRef]
- Yasumura, S.; Hosoya, M.; Yamashita, S.; Kamiya, K.; Abe, M.; Akashi, M.; Kodama, K.; Ozasa, K. Study protocol for the Fukushima Health Management Survey. J. Epidemiol. 2012, 22, 375–383. [Google Scholar] [CrossRef] [Green Version]
- Ohira, T.; Nakano, H.; Okazaki, K.; Hayashi, F.; Nagao, M.; Sakai, A.; Hosoya, M.; Shimabukuro, M.; Takahashi, A.; Kazama, J.J.; et al. Trends in Lifestyle-related Diseases and Their Risk Factors After the Fukushima Daiichi Nuclear Power Plant Accident: Results of the Comprehensive Health Check in the Fukushima Health Management Survey. J. Epidemiol. 2022, 32, S36–S46. [Google Scholar] [CrossRef]
- Maeda, M.; Harigane, M.; Horikoshi, N.; Takebayashi, Y.; Sato, H.; Takahashi, A.; Momoi, M.; Goto, S.; Oikawa, Y.; Mizuki, R.; et al. Long-Term, Community-based Approach for Affected People Having Problems With Mental Health and Lifestyle Issues After the 2011 Fukushima Disaster: The Fukushima Health Management Survey. J. Epidemiol. 2022, 32, S47–S56. [Google Scholar] [CrossRef]
- Ikeda, A.; Steptoe, A.; Shipley, M.; Wilkinson, I.B.; McEniery, C.M.; Tanigawa, T.; Singh-Manoux, A.; Kivimaki, M.; Brunner, E.J. Psychological Wellbeing and Aortic Stiffness. Hypertension 2020, 76, 675–682. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Ohira, T.; Yasumura, S.; Maeda, M.; Otsuru, A.; Harigane, M.; Horikoshi, N.; Suzuki, Y.; Yabe, H.; Nagai, M.; et al. Effects of socioeconomic factors on cardiovascular-related symptoms among residents in Fukushima after the Great East Japan Earthquake: A cross-sectional study using data from the Fukushima Health Management Survey. BMJ Open 2017, 7, e014077. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Ministry of Health, L.a.W.i.J. Standard Medical Examination and Health Guidance Program 2018. Available online: https://www.mhlw.go.jp/file/06-Seisakujouhou-10900000-Kenkoukyoku/00_3.pdf (accessed on 16 February 2018).
- Takayoshi Ohkubo, Y.T.; Asayama, K. Blood pressure measurement guidance program. Jpn. J. Cardiovasc. Dis. Prev. 2021, 56, 239–243. [Google Scholar]
- Kessler, R.C.; Barker, P.R.; Colpe, L.J.; Epstein, J.F.; Gfroerer, J.C.; Hiripi, E.; Howes, M.J.; Normand, S.-L.T.; Manderscheid, R.W.; Walters, E.E.; et al. Screening for serious mental illness in the general population. Arch. Gen. Psychiatry 2003, 60, 184–189. [Google Scholar] [CrossRef]
- Uemura, M.; Ohira, T.; Yasumura, S.; Otsuru, A.; Maeda, M.; Harigane, M.; Horikoshi, N.; Suzuki, Y.; Yabe, H.; Takahashi, H.; et al. Association between psychological distress and dietary intake among evacuees after the Great East Japan Earthquake in a cross-sectional study: The Fukushima Health Management Survey. BMJ Open 2016, 6, e011534. [Google Scholar] [CrossRef]
- Sakurai, K.; Nishi, A.; Kondo, K.; Yanagida, K.; Kawakami, N. Screening performance of K6/K10 and other screening instruments for mood and anxiety disorders in Japan. Psychiatry Clin. Neurosci. 2011, 65, 434–441. [Google Scholar] [CrossRef]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: Validation of an instrument based on ICD-10 criteria. J. Psychosom. Res. 2000, 48, 555–560. [Google Scholar] [CrossRef]
- Cnaan, A.; Laird, N.M.; Slasor, P. Using the general linear mixed model to analyse unbalanced repeated measures and longitudinal data. Stat. Med. 1997, 16, 2349–2380. [Google Scholar] [CrossRef]
- Ikeda, A.; Schwartz, J.; Peters, J.L.; Baccarelli, A.A.; Hoxha, M.; Dioni, L.; Spiro, A.; Sparrow, D.; Vokonas, P.; Kubzansky, L.D. Pessimistic orientation in relation to telomere length in older men: The VA normative aging study. Psychoneuroendocrinology 2014, 42, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Ikeda, A.; Schwartz, J.; Peters, J.L.; Fang, S.; Spiro, A.; Sparrow, D.; Vokonas, P.; Kubzansky, L.D. Optimism in relation to inflammation and endothelial dysfunction in older men. Psychosom. Med. 2011, 73, 664–671. [Google Scholar] [CrossRef]
- Peters, J.L.; Kubzansky, L.D.; Ikeda, A.; Fang, S.C.; Sparrow, D.; Weisskopf, M.G.; Wright, R.O.; Vokonas, P.; Hu, H.; Schwartz, J. Lead concentrations in relation to multiple biomarkers of cardiovascular disease: The Normative Aging Study. Environ. Health Perspect. 2012, 120, 361–366. [Google Scholar] [CrossRef] [PubMed]
- Ohira, T.; Tanigawa, T.; Tabata, M.; Imano, H.; Kitamura, A.; Kiyama, M.; Sato, S.; Okamura, T.; Cui, R.; Koike, K.A.; et al. Effects of habitual alcohol intake on ambulatory blood pressure, heart rate, and its variability among Japanese men. Hypertension 2009, 53, 13–19. [Google Scholar] [CrossRef]
- Cavalcanti, A.N.; Marchi, G.M.; Ambrosano, G.M.B. Statistical results on restorative dentistry experiments: Effect of the interaction between main variables. J. Appl. Oral Sci. 2010, 18, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Kario, K. Disaster hypertension—Its characteristics, mechanism, and management. Circ. J. 2012, 76, 553–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, S.S.; Pio, J.R.; Wong, N.D.; Larson, M.G.; Leip, E.P.; Vasan, R.S.; Levy, D. Predictors of new-onset diastolic and systolic hypertension. Circulation 2005, 111, 1121–1127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Xing, F.; Liu, R.; Liu, L.; Zhu, Y.; Wen, Y.; Sun, W.; Song, Z. Isolated diastolic hypertension associated risk factors among Chinese in Anhui Province, China. Int. J. Environ. Res. Public Health 2015, 12, 4395–4405. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ito, K.; Tomata, Y.; Kogure, M.; Sugawara, Y.; Watanabe, T.; Asaka, T.; Tsuji, I. Housing type after the Great East Japan Earthquake and loss of motor function in elderly victims: A prospective observational study. BMJ Open 2016, 6, e012760. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, E.; Ishikawa-Takata, K.; Murakami, H.; Tsuboyama-Kasaoka, N.; Tsubota-Utsugi, M.; Miyachi, M.; Yokoyama, Y.; Sakata, K.; Kobayashi, S.; Ogawa, A.; et al. Relationships between social factors and physical activity among elderly survivors of the Great East Japan earthquake: A cross-sectional study. BMC Geriatr. 2016, 16, 30. [Google Scholar] [CrossRef] [Green Version]
- Ohira, T.; Hosoya, M.; Yasumura, S.; Satoh, H.; Suzuki, H.; Sakai, A.; Ohtsuru, A.; Kawasaki, Y.; Takahashi, A.; Ozasa, K.; et al. Effect of Evacuation on Body Weight After the Great East Japan Earthquake. Am. J. Prev. Med. 2016, 50, 553–560. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, S.; Nagai, M.; Fukuma, S.; Ohira, T.; Hosoya, M.; Yasumura, S.; Satoh, H.; Suzuki, H.; Sakai, A.; Ohtsuru, A.; et al. Influence of Post-disaster Evacuation on Incidence of Metabolic Syndrome. J. Atheroscler. Thromb. 2017, 24, 327–337. [Google Scholar] [CrossRef] [Green Version]
- Ewing, J.A. Detecting alcoholism. The CAGE questionnaire. JAMA 1984, 252, 1905–1907. [Google Scholar] [CrossRef] [PubMed]
- Orui, M.; Ueda, Y.; Suzuki, Y.; Maeda, M.; Ohira, T.; Yabe, H.; Yasumura, S. The Relationship between Starting to Drink and Psychological Distress, Sleep Disturbance after the Great East Japan Earthquake and Nuclear Disaster: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2017, 14, 1281. [Google Scholar] [CrossRef] [PubMed]
- Nakaya, N.; Nakamura, T.; Tsuchiya, N.; Narita, A.; Tsuji, I.; Hozawa, A.; Tomita, H. Prospect of future housing and risk of psychological distress at 1 year after an earthquake disaster. Psychiatry Clin. Neurosci. 2016, 70, 182–189. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men | Women | |||||
|---|---|---|---|---|---|---|
| Without Living Environment Changes | With Living Environment Changes | p for Difference | Without Living Environment Changes | With Living Environment Changes | p for Difference | |
| Number | 4518 | 10,423 | 5872 | 15,661 | ||
| Age, mean (SD) | 63.4 (14.1) | 58.2 (16.4) | <0.001 | 60.9 (15.0) | 55.0 (16.9) | <0.001 |
| BMI (kg/m2), mean (SD) | 23.9 (3.3) | 24.3 (3.4) | <0.001 | 23.3 (3.7) | 23.2 (3.9) | 0.27 |
| Systolic blood pressure, mean (SD) | 130.0 (16.2) | 128.8 (15.5) | <0.001 | 126.7 (17.0) | 123.5 (17.1) | <0.001 |
| Diastolic blood pressure, mean (SD) | 76.8 (10.6) | 77.4 (10.5) | 0.002 | 74.0 (10.5) | 73.4 (10.7) | <0.001 |
| Antihypertensive medication use, % | 26.9 | 24.0 | <0.001 | 26.1 | 19.4 | <0.001 |
| Hypertension, % | 45.5 | 41.5 | <0.001 | 40.1 | 31.3 | <0.001 |
| High triglycerides, % | 21.6 | 25.8 | <0.001 | 14.5 | 14.3 | 0.69 |
| High LDL cholesterol, % | 35.0 | 38.1 | <0.001 | 47.8 | 44.1 | <0.001 |
| Low HDL cholesterol, % | 24.9 | 24.9 | 0.95 | 27.2 | 22.5 | <0.001 |
| Diabetes, % | 16.8 | 15.8 | 0.14 | 9.3 | 7.8 | <0.001 |
| Smoking Status: | ||||||
| never, % | 30.9 | 28.5 | 0.003 | 86.7 | 79.2 | <0.001 |
| ex-smokers, % | 42.5 | 39.2 | <0.001 | 4.6 | 7.4 | <0.001 |
| current smokers, % | 23.2 | 27.2 | <0.001 | 4.0 | 8.4 | <0.001 |
| Drinking Status: | ||||||
| never, % | 33.1 | 34.5 | 0.09 | 76.7 | 72.5 | <0.001 |
| Occasional drinkers, % | 23.6 | 22.5 | 0.15 | 17.3 | 18.4 | 0.07 |
| current drinkers, % | 42.6 | 41.4 | 0.19 | 4.8 | 7.7 | <0.001 |
| K6 ≥ 13, % | 6.2 | 12.8 | <0.001 | 10.2 | 17.5 | <0.001 |
| Regular physical exercise (yes), % | 60.0 | 55.3 | <0.001 | 54.4 | 47.7 | <0.001 |
| Subjective sufficient sleep (yes), % | 93.1 | 84.0 | <0.001 | 89.9 | 78.9 | <0.001 |
| Hypertension: systolic pressure ≥ 140 mmHg or diastolic pressure ≥ 90 mmHg, and/or antihypertensive medication use | ||||||
| High triglycerides: triglycerides ≥ 150 mg/dL (1.69 mmol/L) | ||||||
| High LDL cholesterol: LDL cholesterol ≥ 140 mg/dL (3.62 mmol/L) or medication use | ||||||
| Low HDL cholesterol: HDL cholesterol < 40 mg/dL (1.03 mmol/L) or medication use | ||||||
| Diabetes: fasting glucose ≥ 126 mg/dL (7.0 mmol/L), or casual blood glucose ≥ 200 mg/dL (11.1 mmol) and/or on treatment or HbA1c ≥ 6.5% Drinking Status: never drinkers: never or rarely, occasional drinkers: sometimes, current drinkers: everyday | ||||||
| Men | Women | |||||
|---|---|---|---|---|---|---|
| Without Living Environment Changes | With Living Environment Changes | Without Living Environment Changes | With Living Environment Changes | |||
| Number | 4518 | 10,423 | 5872 | 15,661 | ||
| Reference | β (95% CI) | p value | Reference | β (95% CI) | p value | |
| Systolic blood pressure | ||||||
| Effect at baseline | 0 | 0.09 (−0.43, 0.61) | 0.73 | 0 | −0.32 (−0.76, 0.12) | 0.15 |
| Time-dependent effect ** | 0 | −0.07 (−0.28, 0.15) | 0.55 | 0 | −0.20 (−0.37, −0.02) | 0.03 * |
| Mean value for 2012 (SD) | 128.7 (0.3) | 129.3 (0.2) | 124.3 (0.2) | 124.4 (0.1) | ||
| Mean value for 2015 (SD) | 128.9 (0.3) | 129.1 (0.2) | 125.3 (0.2) | 124.6 (0.1) | ||
| Diastolic blood pressure | ||||||
| Effect at baseline | 0 | 0.63 (0.26, 1.00) | <0.001 * | 0 | 0.22 (−0.09, 0.53) | 0.16 |
| Time-dependent effect ** | 0 | 0.0001 (−0.15, 0.15) | >0.99 | 0 | 0.02 (−0.11, 0.14) | 0.79 |
| Mean value for 2012 (SD) | 77.3 (0.2) | 77.8 (0.1) | 73.7 (0.1) | 74.0 (0.1) | ||
| Mean value for 2015 (SD) | 75.7 (0.2) | 76.4 (0.1) | 72.7 (0.2) | 73.3 (0.1) | ||
| * p value of interaction with time | ||||||
| ** Time × changes in living environment | ||||||
| Adjusted for age, antihypertensive medication use from 2012 to 2015, current smoking, drinking status, regular physical exercise, subjective sufficient sleep, K6 score, and BMI from 2012 to 2015. The p-value of interaction with time is based on the assessment comparing between reference category (“without living-environment changes”) and other categories by using the linear mixed-effect models. | ||||||
| Men | Women | |||||
|---|---|---|---|---|---|---|
| Without Living Environment Changes (Reference) | With Living Environment Changes | Without Living Environment Changes (Reference) | With Living Environment Changes | |||
| No antihypertensive medication users | ||||||
| Number | 1798 | 4508 | 2730 | 7995 | ||
| β (95% CI) | p value | β (95% CI) | p value | |||
| Systolic blood pressure | ||||||
| Baseline difference | 0 | 1.11 (0.44, 1.79) | 0.001 * | 0 | −0.03 (−0.56, 0.51) | 0.92 |
| Time-dependent difference ** | 0 | −0.30 (−0.57, −0.03) | 0.03 * | 0 | −0.27 (−0.47, −0.06) | 0.01 * |
| Mean value for 2012 (SD) | 125.1 (0.3) | 126.3 (0.2) | 120.3 (0.3) | 120.5 (0.1) | ||
| Mean value for 2015 (SD) | 126.0 (0.3) | 126.2 (0.2) | 121.1 (0.3) | 120.6 (0.2) | ||
| Diastolic blood pressure | ||||||
| Baseline difference | 0 | 0.87 (0.40, 1.35) | <0.001 * | 0 | 0.10 (−0.27, 0.48) | 0.58 |
| Time-dependent difference ** | 0 | −0.02 (−0.22, 0.18) | 0.84 | 0 | 0.08 (−0.07, 0.23) | 0.30 |
| Mean value for 2012 (SD) | 76.2 (0.2) | 76.9 (0.1) | 72.2 (0.2) | 72.4 (0.1) | ||
| Mean value for 2015 (SD) | 75.7 (0.2) | 76.5 (0.2) | 71.6 (0.2) | 72.3 (0.1) | ||
| Antihypertensive medication users | ||||||
| Number | 1216 | 2504 | 1535 | 3042 | ||
| β (95% CI) | p value | β (95% CI) | p value | |||
| Systolic blood pressure | ||||||
| Baseline difference | 0 | −0.97 (−1.75, −0.19) | 0.02 * | 0 | −0.29 (−1.02, 0.45) | 0.45 |
| Time-dependent difference ** | 0 | 0.18 (−0.16, 0.52) | 0.30 | 0 | −0.30 (−0.62, 0.01) | 0.06 * |
| Mean value for 2012 (SD) | 135.7 (0.4) | 135.5 (0.3) | 134.5 (0.3) | 134.8 (0.2) | ||
| Mean value for 2015 (SD) | 132.6 (0.4) | 132.7 (0.2) | 133.1 (0.3) | 132.2 (0.2) | ||
| Diastolic blood pressure | ||||||
| Baseline difference | 0 | 0.46 (−0.08, 1.00) | 0.10 | 0 | 0.97 (0.47, 1.47) | <0.001 * |
| Time-dependent difference ** | 0 | −0.01 (−0.24, 0.22) | 0.92 | 0 | −0.24 (−0.46, −0.03) | 0.02 * |
| Mean value for 2012 (SD) | 79.0 (0.3) | 79.4 (0.2) | 76.8 (0.2) | 78.0 (0.2) | ||
| Mean value for 2015 (SD) | 76.0 (0.2) | 76.6 (0.2) | 75.0 (0.2) | 75.4 (0.2) | ||
| * p value of interaction with time | ||||||
| ** Time × changes in living environment | ||||||
| Adjusted for age, antihypertensive medication use from 2012 to 2015, current smoking, drinking status, regular physical exercise, subjective sufficient sleep, K6 score, and BMI from 2012 to 2015. The p-value of interaction with time is based on the assessment comparing between reference category (“without living environment changes”) and other categories by using the linear mixed-effect models. | ||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ikeda, S.; Ikeda, A.; Ohira, T.; Sakai, A.; Shimabukuro, M.; Maeda, M.; Yabe, H.; Nagao, M.; Yasumura, S.; Ohto, H.; et al. Longitudinal Trends in Blood Pressure Associated with The Changes in Living Environment Caused by the Great East Japan Earthquake: The Fukushima Health Management Survey. Int. J. Environ. Res. Public Health 2023, 20, 857. https://doi.org/10.3390/ijerph20010857
Ikeda S, Ikeda A, Ohira T, Sakai A, Shimabukuro M, Maeda M, Yabe H, Nagao M, Yasumura S, Ohto H, et al. Longitudinal Trends in Blood Pressure Associated with The Changes in Living Environment Caused by the Great East Japan Earthquake: The Fukushima Health Management Survey. International Journal of Environmental Research and Public Health. 2023; 20(1):857. https://doi.org/10.3390/ijerph20010857
Chicago/Turabian StyleIkeda, Satomi, Ai Ikeda, Tetsuya Ohira, Akira Sakai, Michio Shimabukuro, Masaharu Maeda, Hirooki Yabe, Masanori Nagao, Seiji Yasumura, Hitoshi Ohto, and et al. 2023. "Longitudinal Trends in Blood Pressure Associated with The Changes in Living Environment Caused by the Great East Japan Earthquake: The Fukushima Health Management Survey" International Journal of Environmental Research and Public Health 20, no. 1: 857. https://doi.org/10.3390/ijerph20010857