Sexual Dimorphism in Human Sacrum in Western (UP) Population Using MDCT
Sexual Dimorphism in Human Sacrum in Western (UP) Population Using MDCT
Volume 9, Issue 11, November – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24NOV1323
Sexual Dimorphism in Human Sacrum in Western
(UP) Population using MDCT
Waseem Ahmad1
Lecturer, Tahira khanam’s Institute of Paramedical Sciences,
Srinagar Jammu and Kashmir, India
Mamta Verma2*
Assistant Professor,
Department of Radiological Imaging Techniques,
College of Paramedical Sciences, Teerthanker Mahaveer University,
Moradabad, UP,India.
Corresponding Author: Mamta Verma2*
Abstract:- I. INTRODUCTION
Objective: CT (computed tomography) is anticipated on the basic
The objective of this study was to evaluate the role of rule that the thickness of the tissue passed by the x- ray shaft
3D CT in Forensic Radiology for gender estimation and is regularly estimated from the computation of the attenuation
toestimate the difference in curvature between male and coefficient.
female sacrum using volume rendering.
A. Principle of Computed Tomography
Methods: The fundamental standard behind CT is that the inward
A total of 30 patients from known age (20-60) which structure of an article can be remade from various projections
include 17 males and 13 females these patients were taken of the object.
from teerthanker mahaveer hospital and research center,
all the patients reffered for CT L-S spine. All the patients 3D volume rendering, is the post processing technique
fulfilling inclusion criteria for scan to be done 2D images and produce 3D images that have a better image quality.
were then converted in 3D data by using IRS technique,
various measurements were done from MPR and 3D Multiplanar reformation, is the process of using data
image. from axial CT image to create non axial two dimensional.1
Results: B. Multi-Slice Computed Tomography
From all the studied measurements, were as L-S The Multi-Slice CT (MSCT) is a CT framework
Angle , Anterior sacral Angle, Sacral Base Angle, height, furnished with various lines of CT finders to make pictures of
width and curvature of the sacrum. In this study LSA and numerous segments. This CT framework has various
SBA was found higher in females than males, also it was attributes from customary CT frameworks, which have only
found that curvature and width of sacrum was higher in one line of CT finders. The presentation of this propelled
females, ASA and height of sacrum found higher in males identifier framework and its blend with helical filtering has
as compered to females. notably improved the exhibition of CT as far as imaging
range, time for assessment, and picture resolution.
Conclusion:
After completion of study it was concluded that the C. Image Reconstruction Technique
prevalence of male case was higher than that of female Picture reproduction in CT might be a numerical activity
cases according to the present study. In the persent study that produces tomographic pictures from X-beam projection
the various parameters of the sacral index were found to information obtained at different edges round the patient.
be significant assocated with respect to the gender. Picture remaking impactsly affects picture quality and in this
way on radiation dose.An calculation is a numerical strategy
Keywords:- Lumbosacral Spine, Multiplanar Reconstruction, for comprehending a problem.the following three scientific
Multi detector Computed Tomograpy, Image Reconstruction techniques for picture recreation will be depicted:
system, Three dimensional, Sacral Base Angle, Anterior
Sacral Angle, L-S Angle.
IJISRT24NOV1323 www.ijisrt.com 1434
Volume 9, Issue 11, November – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24NOV1323
Back Projection D. Sacrum Anatomy
Back projection sometimes called ‘summation method’ The name sacrum is gotten from the Latin and Greek
is the oldest means of image reconstruction .None of the underlying foundations of os sacrum which means hallowed
commercial CT scanners uses simple back projection ,but it bone.
is the easiest method to describe so we will use it as prototype.
The human sacrum is a huge triangular combined bone
Iterative Methods of five separate vertebras that wires alongside the mediating
An iterative remaking begins with a presumption (for intervertebral plates, shapes the postero-superior mass of
instance, that all focuses in the network have and contrasts pelvic hole, Wedged between the two innominate bones. The
this suspicion and estimated values makes amendments to sacrum offers backing to the erect prostrate and assists with
bring the two into understanding and afterward rehashes the giving security and solidarity to the pelvis during the
procedure again and again until the expected and estimated transmission of burdens from the hub spine to the pelvic
values are the equivalent or inside satisfactory limits.There girdle.The sacrum verbalizes with four bones; the upper piece
are three varieties of iterative reproductions, contingent upon of the sacrum is associated with the last lumbar vertebra
whether the remedy grouping includes the whole lattice, one above by means of a circle space and feature joint complex,
beam, or one point. as a rule it starts when the five unfused vertebra begin
melding at the age of 16-18 years and finishes its combination
Simultaneous Reconstruction arranges a solitary bone at 34 years old years. The three
All projections for the whole grid are determined toward distinct surfaces of sacrum which are formed to oblige
the start of the cycle, and all redresses are made at the same different structures.the state of the sacrum bone is raised
time for emphasis. looking ahead and it is curevd upon itself set sideways .in
chilhood individual sacral vertebrae are associated via
Ray- by-Ray Correction ligament and detachable by maceration. The grown-up bone
One beam entirety is determined and revised and these holds numerous vertebral highlights. It comprises of base,
amendments are consolidated into future beam wholes with pelvic dorsal and horizontal surfaces, sacral zenith and sacral
the technique being rehashed for every single beam in every cannal.
cycle.
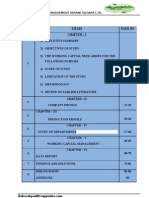
Base of Sacrum( Fig.1)
Point-by Point Correction It is shaped by the upper surface of S1.the body is
The computations and remedies are made for all beams enormous and more extensive transversely, its front
going through one point and these rectifications are utilized projection edge the sacral projection. The vertebral foramen
in resulting counts again with the procedure being rehashed is triangular, its pedicle being short and dissimilar
for each point. posterolaterally. The laminae are slanted, coordinated
posteromedially to meet at spinous tubercle. Better articular
Analytic Methods procedures coordinated posteromedially than articulate with
Explanatory strategies diagnostic techniques are utilized sub-par articular procedure of L5. Transverse procedure is
in practically all X- raybeam CT today. These calculations abroad slanting mass tasks along the side from the body,
vary from iterative strategies in that careful equations are pedicle and unrivaled articular procedure are interesting
used for the explanatory reproductions. These equations are highlights of sacrum. The transverse procedure and costal
alarmingly unpredictable to most radiologists despite the fact components are combined togetherto the remainder of the
that mathematicians state they are actually very basic. We vertebrae shaping the predominant piece of the sacral
will just endeavor a pictorial clarification of the two horizontal mass or ala.
mainstream scientific techniques two-dimensional Fourier
investigation and separated back projection. . Sacrum pelvic surface(Fig.2)
Faces antero-inferiorly, It is vertical and transversely
Two-Dimensional Fourier Analysis inward. Be that as it may , S2 may create a convexity. Four
The premise of Fourier investigation is that any capacity sets of pelvic sacral foramina with the sacrum cannal,
of time or space can be spoken to by the entirety of different transmitting ventral rami of upper 4 sacral spine nerves. The
frequencies and amplitudes of sine and cosine waves. enormous region among right and left foramina, framed by
level pelvic parts of the sacrum bodies shows their
Filtered Back-Projection combination by 4 transverse edges. The bars between
Sifted back projection is like back-projection aside from foramina are the costal components,combined to the
that the picture is separated or adjusted,to precisely offset the vertebrae. The parallel piece of the sacrum is armed by the
impact of abrupt thickness changes which causes obscuring combination of costal components with transverse
in basic back projection.2 procedures.
IJISRT24NOV1323 www.ijisrt.com 1435
Volume 9, Issue 11, November – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24NOV1323
Sacrum Dorsal Surface (Fig.3) C. Inclusion Criteria:
Sacrum dorsum surface is raised and pretender
prevalent. It has a rised intruded on, middle sacral peak with Patients of western (UP) population of age group 20-
4 spinous tubercules speaking to intertwined sacral spines. 60years
Beneath the fourth or third a curved sacral rest is available in Patient referred for CT L-S Spine and Pelvic CT
the back mass of the sacral channel which is because of Both male and female patients
disappointment of the fifth pair of laminae to meet, in the Female patients need to fulfill 10 day rule
inside uncovering the dorsal surface of fifth sacral body. Previous normal data can be retrieved from the system
Horizontal to the middle peak are the 4 sets of dorsal foramina
which lead into the sacral cannal through intrervertebral D. Exclusion Criteria:
foramina, each transmitting the dorsal ramus of a sacral spinal
nerve. Average to the foramina, vertically underneath each Trauma cases are excluded
articular procedure lays 4 msall tubercles all things
Patient with pot’s, metastasis are not included
considered called the moderate sacal peak.
E. Sample Size:
The fifth mediocre aticular process extends caudally and
We used appropriated routinely protocol for CT L-S
flanks the sacral break as sacral cornua. Sidelong to the dorsal spine. A total of 30 patients (Age 20-60) are included in this
sacral foramina is a horizontal sacral peak, framed by the
study to differenciate in curvature between male and female.
intertwined transverse procedures, whose apices show up asa
sample who visited in Teerthanker Mahaveer hospital for
line of transverse tubercles.
their diagnosis in CT modality.
Sacrum Lateral Surfaces (Fig.4) F. Technique of Examination:
This is the combination of transverse procedures and
All patients are screened before entry into the CT
costal components which are wide above and tight beneath.
scanner room for metallic objects of the interest of part.
The wide upper part bears an auricular surface for explanation
Patients were examined in the supine position on the patient
with ilum which resembles a reversed last 'L' . The shorter
table with proper positioning .The L-S spine protocol 4 initial
cranial appendage is confined to the S1 and caudal appendage
topogram of the L-S spine has obtained. CT L-S spine
slipping upto the center of S3. Past this the sidelong surface protocol ( Tabl 1) at 128 slice includes the spine , set the
is non – articular and decreased in expansiveness. Caudally it
protocol (KVp, mA, slice thickness, Interslice gap etc.),
bends medially to the collection of S5 at the second rate
protocol also include axial plain with 3 mm slice thickness,
parallel edge. Past which the surface becoms a slender
there by reconstruction, post processing and reformatting
parallel outskirt. The auricular surface shows cranial and
images into multiple planes.
caudal rise a halfway melancholy.
To find the accuracy of gender estimation by taking
Sacral Apex
various measurements of the following parameters
The inferior aspect of body of S5which bears an ovel
It would be helpful in forensic department to identify the
facet for the articulation with coccyx.
damaged \degraded body with their sacrum
Sacral Canal
L-S Angle
framed by the sacral vertebral foramina, it is triangular
Sacral base angle
in segment. Basal opening is diagonal because of sacral
Anterior sacral angle
tendency, is derected cranially in the standing position. Every
horizontal divider presents 4 intervertebral formaina, through
which they are continous with pelvic and dorsal sacral Diameter
foramina. Its caudal opening is the sacral rest.3
Max. height
II. METHODS Max width
The study was conducted at Department of Radiology, Curvature
Moradabad.
Anterior
A. Type of the Study:
Retrospective study. All the patients fulfilling inclusion criteria will be
informed and instructed for the scan to be done. 2D images
B. Setting: then will be converted to 3D data by using Image
It is a retrospective study that was conducted over 1 year reconstruction technique. Various sacrum parameter
at the Radiology department of Teerthanker Mahaveer measurements ( Table 2) will be taken from MPR and 3D
hospital Moradabad U.P. This study carried out on PHILIPS image.All the collected data will further be send for statistical
INGENUITY CORE 128 slice CT Machine. analysis.
IJISRT24NOV1323 www.ijisrt.com 1436
Volume 9, Issue 11, November – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24NOV1323
G. Data Management Statistical Analysis: 35.552±5.682. Therefore, a significant association was
The data was collected and entered in MS excel 2013. observed between the parameters like LSA, SBA and ASA
Different Diverse measurable examination was performed with p-value <0.05 (CI -95%). The mean ± Std. Deviation of
utilizing SPSS programming rendition 22. The one sample other parameters like Height, width and curvature in female
Kolomogorov - Smirnov Test will be employed to determine cases were found to be 8.953±0.602, 11.5323±0.600 and
whether the data sets different from a normal distribution or 129.4±5.7373 respectively whereas in male cases the mean ±
not .Descriptive statistics will be calculated for quantitative Std. Deviation of parameters like Height, width and curvature
variables. was found to be 10.117±1.091, 10.754±0.480 and
123.441±7.907 respectively(Table 5 and Graph 2 )A
Wilcoxon test for significant risk factors were done by significant association was observed between these
logistic regression method. parameters and the gender (p-value <0.05).
In result, If p<0.05 then hypothesis is said to be IV. DISCUSSION
statistically significant and if p>0.05, then hypothesis is said
to be statistically insignificant. In the present study, as per the several sacral parameters
amongst different population groups, it was observed that the
III. RESULT mean of LSA, SBA and ASA was higher in female cases as
compared to that of male cases. Similar to our study, the
After CT L-S Spine procedure out the inclusion criteria, results revealed by the study conducted by Davivongs et al.5
a total 30 patients of both gender and different age group has shown that the sacral index was more in females than that
were included in the present retrospective study. An informed of males. Another study conducted by Kumar A et al.6 also
consent was obtained from all the patients before they were showed that the mean sacral index was higher in females.
subjected for evaluation. Out of 30 patients are included in Hence it can be summarised from the present study that the
this study, 13/30 (44%) patients females and 17/30 (56%) most of the values for the parameters like LSA, SBA, ASA,
patients males. Maximum number of MDCT patients was in the width as well as the anterior and posterior curavature were
the age group of 20-60 Years .Table 3 & Graph 1 show the higher in females whereas the other parameters like the height
gender-wise distribution of the study subjects illustrating the was higher in male cases. However, according to a study
frequencies . The prevalence of male cases (56.7%) was conducted by Frazer et al.7, it is revealed that as compared to
higher than female cases (43.3%). the male cases, the bone of females is broader, showing a
different curve anteriorly. In males the bend is less or
The present study was an attempt to estimate the progressively uniform from above downwards though if there
difference in curvature between male and female sacrum should arise an occurrence of females it is stamped pointedly
using volume rendering and to evaluate the role of 3D CT in at the lower part. As shown in our present study the value of
forensic radiology for gender estimation according to the the curvature was found to be higher in females. Similar
available data of thirty cases with relation to the various findings were seen in the sacrum studied by Kanika et
parmeters. The various parameters were selected on the basis al.8 ,Mishra et al.9,Sachdeva et al.10 Steyn et al.11Abhimanyu
of various reviews of literatures. In the present retrospective et al.12 , Sibani Mazumdar et al.13 , Renuka et al.14 Raju et
study, which was conducted at TeerthankerMahaveer al.15.The sacrum is more curved in men than in women.
Hospital & Research Centre, recruited a total of thirty cases
consisting of 17 male cases followed by 13 female cases.
V. CONCLUSION
For all the parameters taken under consideration, the
mean, standard deviation and interquartile range were The present study aimed at estimating the difference in
depicted. As per the overall variability of the study subjects, curvature between male and female sacrum using volume
the mean age and the standard deviation was found to be rendering and in evaluating the role of 3D CT in forensic
30.09 and 8.298 (with the interquartile range = 11). The mean radiology for gender estimation. The prevalence of male
of Lumbo sacral angle was found to be 52.74 with the cases was higher according to the present study.
standard deviation of 5.21 whereas the mean Anterior Sacral
angle was found to be 57.68 with the standard deviation of In the human skeletal framework, the distinguishing
3.208 (Interquartile range=2.92). Moreover, the mean Sacral proof of gender turns out to be progressively significant as
Base angle was 37.18 with the standard deviation of 5.960 sacrum is a segment of pelvic support with utilitarian
(Interquartile range=5.960) (Table 4) contrasts between the two gender. In the present study the
various parameters of sacral index like LSA, SBA, ASA,
According to the gender-wise comparison of the study height width and the anterior curvature were found to be
population, in case of female patients the mean ± Std. significantly associated with respect to the gender.
Deviation of LSA was found to be 55.346±3.68, the mean ±
Std. Deviation of ASA was 56.215±1.937, the mean ± Std. Amongst all the indices, the height was found to be the
Deviation of SBA was 39.315±5.841 whereas in male cases most significant factor associated with both gender. The
the mean ± Std. Deviation of LSA was found to be anterior curavatures were broader in females as compared to
50.759±5.4217, the mean ± Std. Deviation of ASA was male cases which were preferably similar to the
58.811±3.569, the mean ± Std. Deviation of SBA was investigations done by several investigators.
IJISRT24NOV1323 www.ijisrt.com 1437
Volume 9, Issue 11, November – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24NOV1323
Hence, the present study suggests that during the
surgical procedures, these parameters must be taken foremost
under consideration. Moreover, the analysis of human sacrum
can be used as a supportive finding in the estimation of the
differences in the curvature. Furthermore, more studies can
be done using a large sample sizes for the efficient
observations.
REFERENCES
[1]. Euclid Seeram, "Computed Tomography" Physical
Principals, Clinical Applications, andQuality Control
Third Edition; Copyright 2009 page no 2
[2]. Satish k. Bhargava ,Fourth Edition Textbook of
radiology for resident and technicians, page no 108
[3]. Gray, Henry. Anatomy of the Human
Body. Philadelphia: Lea & Febiger, 1918;
Bartleby.com, 2000. www.bartleby.com/107/
[4]. Sumeet Bhargava .CT and MRI Protocal a practical
Approach Third Edition; Copyright 2018 page no 110
[5]. Davivongs V, The pelvic girdle of the Australian
Aborigine; sex differences and sex determination, Am
J PhysAnthropol, 1963; 21: 443-56.
[6]. Kumar A et al. An Anthropometric Analysis of Dry
Human Sacrum: Gender Discrimination, International
Journal of Science and Research (IJSR) 2013; vol
4(4).
[7]. J.E. Frazer, Anatomy of human skeleton 3rd Edition,
1933; 43.
[8]. S Kanika et al, Role of Sacrum in Sexual Dimorphism-
A Morphometric Study. J Indian Acad Forensic Med,
July-September 2011; Volu 33(3) ISSN 0971-0973.
[9]. Mishra SR, Singh PJ, Agrawal AK, Gupta RN,
Identification of sex of sacrum of Agra region. J
AnatSoc Ind. 2003; 52(2): 132-136.
[10]. Sachdeva K, Singla RK, Kalsey G, Sharma G. Role of
Sacrum in sexual Dimorphism – A morphometric
study. J Indian Acad Forensic Med.,2011; 33(3):206-
210.
[11]. Steyn M, Işcan MY, Metric sex determination from
the pelvis in modern Greeks, Forensic Science
International. 2008; 179:86-89.
[12]. . Abhimanyu Pradhan, Sushil Yadav; Sexual
dimorphism of the sacrum in south Indian population
using MRI ; Indian Journal of Pharmacy and Bio
Science ; 2015 ; 6(4) ; 398-404
[13]. Sibani Mazumdar, Ansuman Ray, Ardhendu
Mazumda, Sudeshna Majumdar, Abhik Sinha, Sanjoy
Vasisht; Sexual dimorphism and regional difference in
size of sacrum, a study in wastern India US National
library of Medicine enlisted journal; 2012; 5(3); 298-
307
[14]. Renuka s Ahnakari ,MP ambali ; Sexual dimorphism
in human sacrum in Maharashtra population ;
international journal of Clinical Anatomy and
Physiology; 2016; 3(1) ;91-96.
[15]. Raju PB, Singh S, Padmanabhan R. Sex determination
and sacrum. J AnatSoc Ind. 1980; 30(1): 13-15.
IJISRT24NOV1323 www.ijisrt.com 1438
Volume 9, Issue 11, November – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24NOV1323
Fig.2: Sacrum, pelvic surface
Fig 1: Base of Sacrum
Fig 2: Sacrum Pelvic Surface
IJISRT24NOV1323 www.ijisrt.com 1439
Volume 9, Issue 11, November – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24NOV1323
Fig 3: Sacrum, Dorsal Surface
Fig 4: Lateral Surfaces of Sacrum
IJISRT24NOV1323 www.ijisrt.com 1440
Volume 9, Issue 11, November – 2024 International Journal of Innovative Science and Research Technology
ISSN No:-2456-2165 https://doi.org/10.38124/ijisrt/IJISRT24NOV1323
TABLES
Table 1: CT Protocol for L-S Spine
L-S SPINE
Protocol Spine helical
Patient position Spine feet first
Scano 1800 DUAL Scout
Area coverage Spine
Scan direction Crania caudal
Routine plain
Collimation 64X 0.625
Slice thickness 3mm
Increment 3mm
Kv,mAs/slice 140,250
Resolution Standard, Filter, sharp,
Table 2: Parameters of Sacrum Measurements
Parameters Measurements
Lumbo sacral angle The edge between the foremost fringe of s1 vertebral body and that of the fifth lumbar
(LSA) vertebral
Sacral base angle The edge between the unrivaled fringe of s1 vertebral body and the even line
(SBA)
Anterior sacral angle The edge between the unrivaled and foremost fringes of s1 vertebral body
(ASA)
Maximum height The hight was estimated along the center of anterio better edge of promontary than center of
antero sub-par edge of last sacral vertebra
Maximum width The width was estimated from the sidelong most piece of alae of sacrum at the upper piece of
auricular surface and the separation was estimated along foremost part of sacrum at the degree
of Ist sacral vertebra
Anterior curvature it was measured by taking maximum height of sacrum /curvature length of sacrum ×100
Table 3: Gender-Wise Distribution of the Study Subjects (N=30)
Gender Frequency (f) Percent (%)
Female 13 43.3
Male 17 56.7
Table 4: Representation of Mean with Variability and Interquartile Range in the Sample Characteristics
Variables Mean ± Std. Deviation Interquartile Range
Age 30.9±8.298 11
LSA (degree) 52.74667±5.212 7.1
ASA (degree) 57.68667±3.208 2.92
BSA (degree) 37.18333±5.960 7.85
Max Height (cm) 9.613333±1.07 1.13
Max Width (cm) 11.09133±0.656 1.15
Curvature (mm) 126.0233±7.559 11.8
Table 5: Gender Wise Comparison of Various Parameters of Sacrum
Variables Mean ± Std. Deviation P-value
Female Male (CI -95%)
LSA (degree) 55.346±3.68 50.759±5.4217 0.014
ASA (degree) 56.215±1.937 58.811±3.569 0.036
BSA (degree) 39.315±5.841 35.552±5.682 0.038
Max Height (cm) 8.953±0.602 10.117±1.091 0.001
Max Width (cm) 11.5323±0.600 10.754±0.480 0.003
Curvature (mm) 129.4±5.7373 123.441±7.907 0.044