Measuring the
Mandates
Questioning the State’s
Response to COVID-19
Index
One. Pandemic or Democide: What Caused the Excess Deaths?
Introduction
‘In the past politicians promised to create a better world. They had different ways of achieving this, but their power and authority came from the optimistic visions they offered their people. Those dreams failed, and today people have lost faith in ideologies. Increasingly, politicians are seen simply as managers of public life, but now, they have discovered a new role that restores their power and authority. Instead of delivering dreams, politicians now promise to protect us—from nightmares.’
Adam Curtis1
The above quotation is from Adam Curtis’ documentary series, The Power of Nightmares. In the next line Curtis states that politicians:
‘Say that they will rescue us from dreadful dangers that we cannot see and do not understand.’
Given the context of this document, you would be forgiven for thinking that The Power of Nightmares is a documentary criticising the political response to COVID-19. It is not. Produced in the aftermath of September 11th, it is actually about the nightmare of international terrorism. On a deeper level however, Curtis’ work is about COVID-19. It is about financial crises, drug trafficking and violent crime too. If we look beyond his specific example, it is about all claims that the state is the sole entity capable of protecting us from such evils.
In 2020, the announcement of a pandemic saw the implications of this claim manifest in the most pronounced and consequential manner since the Second World War. Politicians around the world insisted that they needed to restrict human freedom and mandate medical interventions—all in order to keep us safe. They had the power and claimed the wisdom to know this was the right thing to do. Much of the population agreed, yearning only for stronger restrictions on their liberty.
The human cost of these policies has been as horrendous as it was predictable—a fact not even their most ardent defenders can seriously contest. We’ve witnessed the closing down of businesses, the coercion of medical treatments, the loss of jobs, the separation of families, elderly people dying alone in care homes and starvation levels increasing around the world. For this, we have been landed with a bill that we will be paying off for generations to come.
Yet much like the Great Wars of the 20th century, the argument goes that if the state hadn’t intervened the situation would have been much worse. The implementation of these draconian measures means that millions of people are now alive who otherwise wouldn’t have been. However brutal, the price was worth it.
Is this position defensible? Were any of the state mandates actually justified, even given the limited information available at the time? With hindsight, were they beneficial, or did they end up making matters worse? If they did worsen the situation, are there a different set of general principles that politicians could be guided by when future nightmares arise? These are the questions this document seeks to address.
About this Document
This document is an international version of one originally created for submission to an inquiry on the Isle of Man. It was composed by citizens who share a deep concern over how states responded to COVID-19, and what the implications of that response herald for the future. These concerns centre around the issue of mandates: the unprecedented coercing of behaviour that began in March of 2020. This document is intended to question whether these mandates succeeded even on their own terms.
Quotations, especially those taken from speech, have sometimes been slightly altered to favour readability. The meaning is never affected. An effort has been made to—wherever possible—provide sources that are openly accessible on the internet.
If this document proves helpful, the reader is at liberty to republish any part of it they wish to, or submit it to their own nation's inquiries.
Inquiries regarding the report can be made at: https://www.deepstateconsciousness.com/contact
One. Pandemic or Democide: What Caused the Excess Deaths?
‘Democide means for governments what murder means for an individual under municipal law. It is the premeditated killing of a person in cold blood, or causing the death of a person through reckless and wanton disregard for their life.’
Rudolph Rummel1
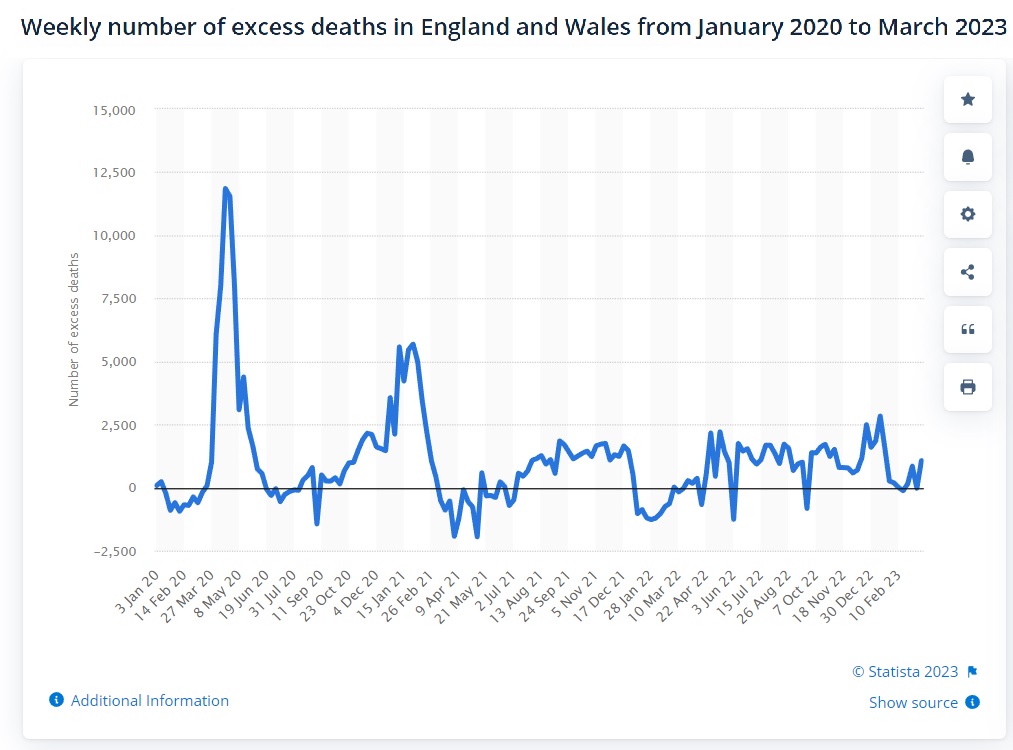
For many people, any initial feelings of cynicism regarding the dangers of COVID-19 dispersed in April of 2020, when excess mortality figures suddenly spiked around the world. England and Wales experienced nearly sixty thousand excess deaths during a three month period:2
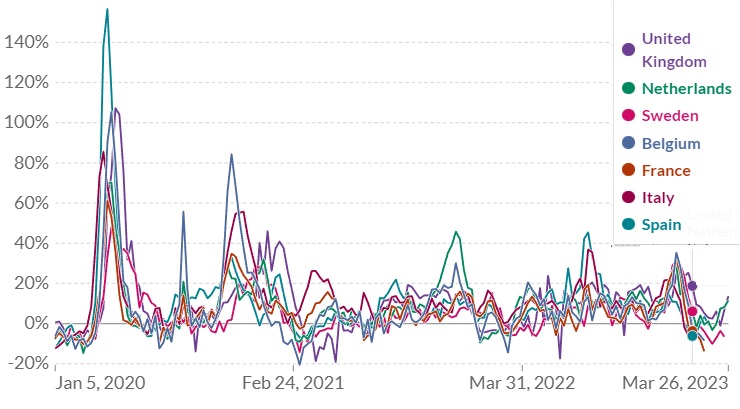
At the same time, excess mortality spiked across various European countries:3
The identification of a novel coronavirus had been announced by the world’s media, then suddenly vast numbers of people started dying across multiple countries. Whilst correlation alone does not prove causation, surely the new virus must be the sole culprit for these deaths.
Two voices that were early in cautioning against an unguarded leap to such a conclusion were Dr. Claus Köhnlein and journalist Torsten Engelbrecht. Köhnlein and Engelbrecht are co-authors of the book Virus Mania,4 which critically examines the foundations and assumptions of virology. In an article published in October of 2020, they claimed that a comparison of excess mortality across countries actively disproved the viral hypothesis.5
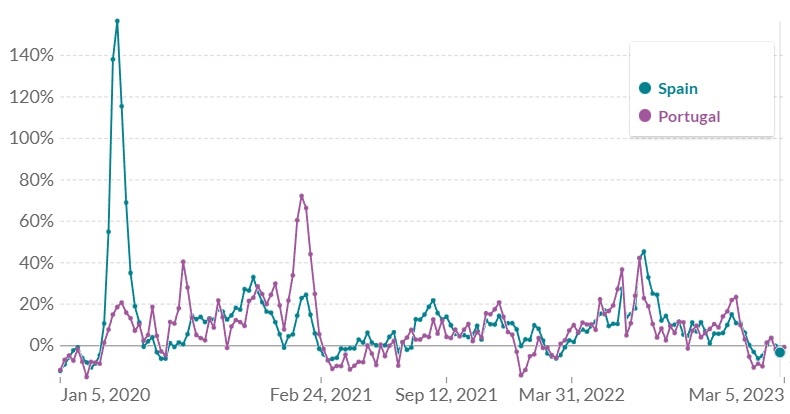
They point out the striking contrast between neighbouring countries Spain and Portugal, where the former had 157% excess deaths, at the same time the latter’s peaked at 21%:6
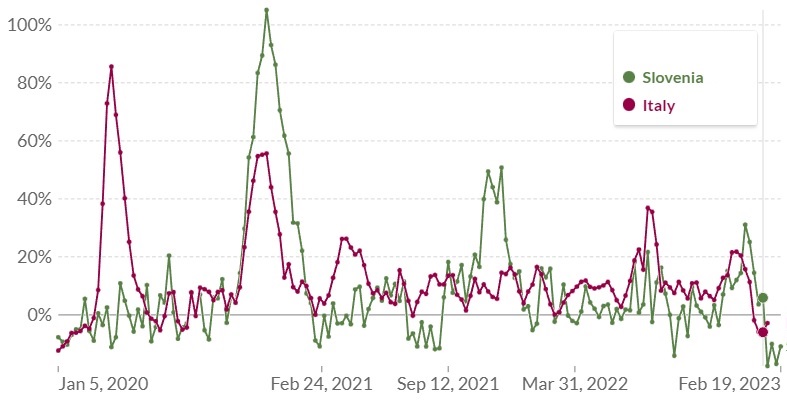
The same situation exists between Italy and Slovenia. During this initial period, Italian excess mortality peaked at 86%, whilst the Slovenian reached 11%. Italy’s excess was entirely concentrated in the North of the country, where Bergamo reached a 1,000% excess.7
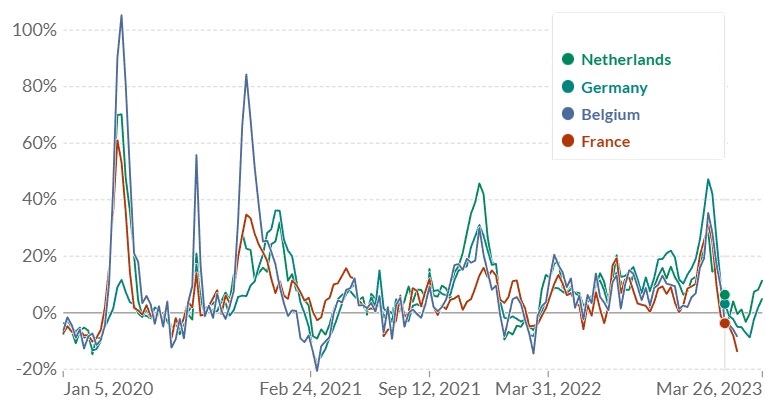
Germany also contrasts sharply with her high excess neighbours. Belgium's excess peaked at 105%, the Netherlands was 70, whilst France hit 61. Germany’s only reached 12% during this initial period.8
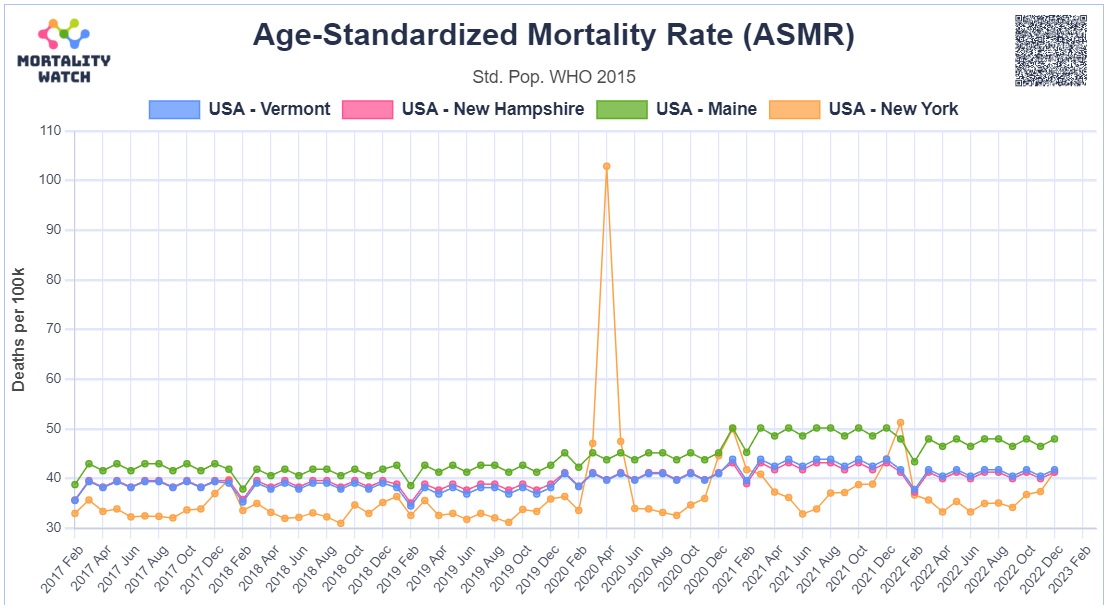
A similar picture emerges in the United States. At the time New York was experiencing an over 130% increase in excess mortality (over 630% in some parts of New York City), neighbouring Vermont and nearby New Hampshire and Maine experienced little to no excess:9
Köhnlein and Engelbrecht assert that:
‘A virus pandemic, which afflicts countries so differently, cannot actually exist, especially in today’s times.’10
Is this true? Köhnlein and Engelbrecht provide no comparison to historical data to support their claim. Making such a comparison would also be difficult, due to the unprecedented steps taken to counteract COVID-19. We were truly living through unique times. The data is perhaps intriguing enough however, to at least look and see if any other factors could have been feeding into the excess mortality.
Out of concern for this situation, Claus Köhnlein submitted a letter to the German Ärzteblatt medical journal, stating:
‘In view of the fact that very different mortality rates are reported in different European countries, it is reasonable to assume that a differently aggressive therapy could be responsible for this.’11
Köhnlein and Engelbrecht focus on drug trials, stating that:
‘This is why there can only be a non-viral explanation for this temporary massive excess mortality. And there is solid evidence that the massive and high-dose administration of highly toxic drugs plays the decisive role—drugs that have been used in worldwide trials and also beyond these trials, costing the lives of tens of thousands of test persons. In the course of time the “patient supply” dried up which explains the rapid drop in the curves creating these “prongs.”’12
In opposition to the viral hypothesis, this position has become known as the iatrogenic (medically induced) hypothesis of COVID-19.
In a paper supporting the iatrogenic hypothesis, Dr. Denis Rancourt draws attention to comments made by World Health Organization (WHO) Director-General Dr. Tedros Adhanom Ghebreyesus, on March 11th 2020, when declaring a pandemic:13
‘I remind all countries that we are calling on you to activate and scale up your emergency response mechanisms; communicate with your people about the risks and how they can protect themselves – this is everybody’s business; find, isolate, test and treat every case and trace every contact; ready your hospitals; protect and train your health workers.’14 [emphasis added]
Tedros Adhanom’s advice is consistent with WHO pandemic preparedness documents.15
The COVID-19 virus is reckoned to have been spreading over the world for months at this point, yet there was no sign of excess mortality anywhere except possibly China.16 Immediately after the WHO declares a pandemic and makes reference to making hospitals ready, the death rate dramatically spikes in various European countries, US States and Canadian provinces. These spikes are unprecedented in both their scale and the fact that they take place outside of the usual flu season. They occur simultaneously in geographic areas separated by thousands of miles, yet not necessarily in neighbouring countries or even provinces.
Various explanations are offered as to how the virus could spread without noticeably affecting mortality rates, then suddenly transform itself into the worst killer in a century.17 None of these explanations can account for the WHO’s seeming ability to predict the onset. Dr. Rancourt proposes that it is far more likely that the excess mortality was due to the implementation of pandemic preparedness across the regions that suffered with it.18
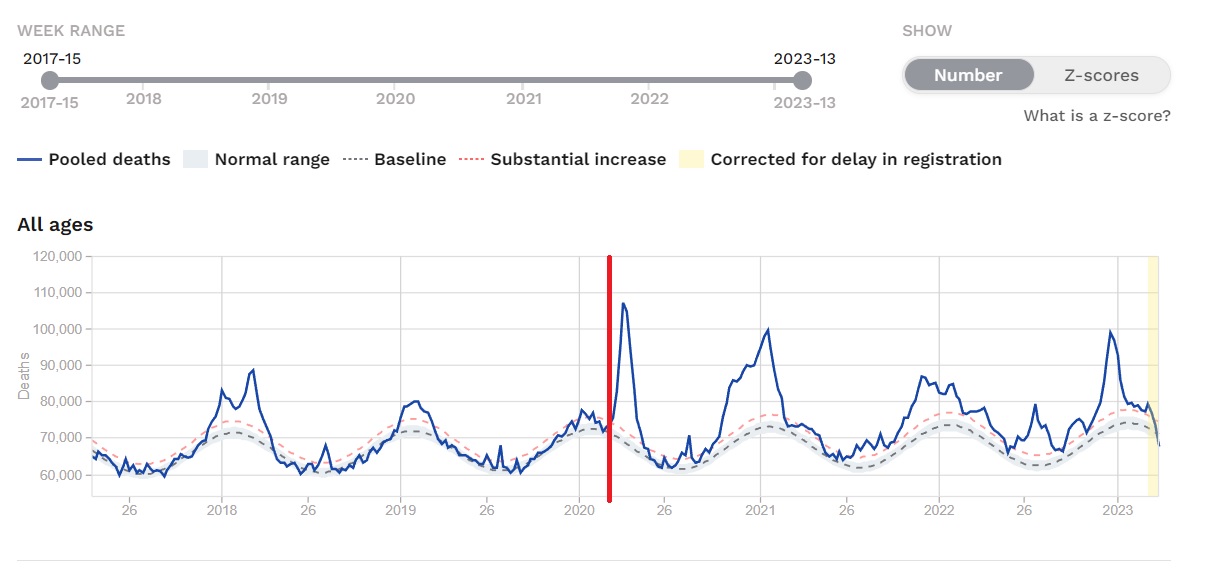
This is the excess mortality for all of Europe, with a red line added to indicate the date of the WHO announcement.19
And this is the United States:20
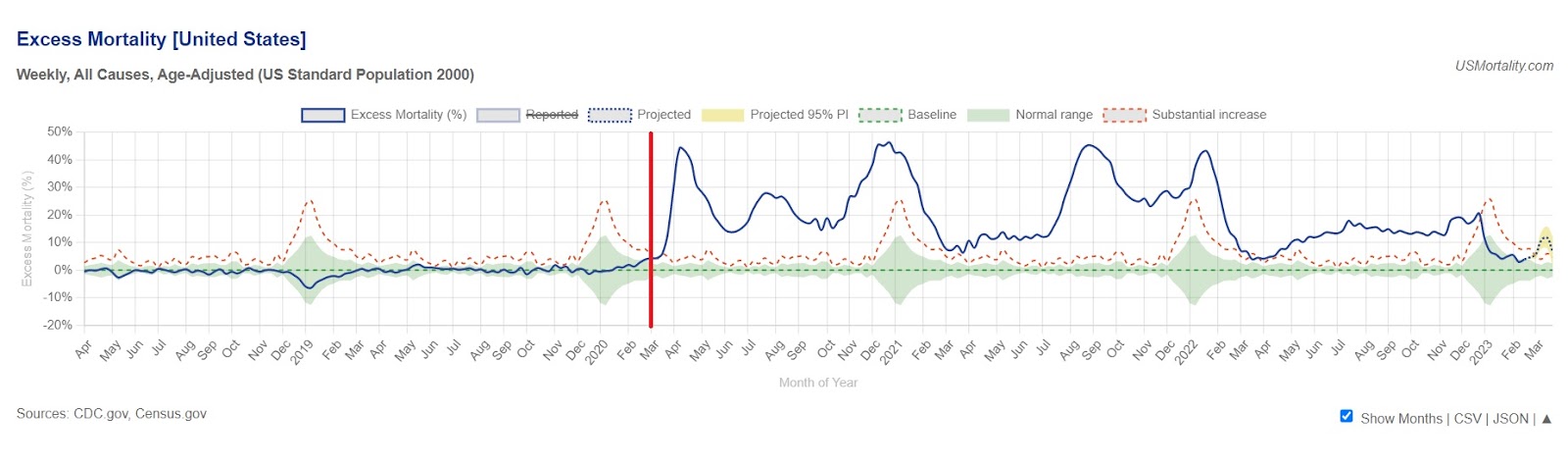
Although COVID-19 was apparently circulating, there was simply no excess prior to this point outside of the annual flu season. Europe is more similar to the United States than France is to Germany, Spain to Portugal, or New York to Vermont.
We will now examine what the various implications of readying hospitals were for excess mortality.
Denial of access to hospitals and other medical services
In October of 2020 Amnesty International published a report titled As if Expendable: The UK Government’s Failure to Protect Older People in Care Homes During the COVID-19 Pandemic.21 It makes for a truly harrowing read. Amongst many issues, the report highlights elderly people being refused medical care after the declaration of a pandemic:
‘Amnesty International has received multiple reports of care home residents’ right to NHS services, including access to general medical services (GMS) and hospital admission, being denied during the pandemic, violating their right to health and potentially their right to life, as well as their right to non-discrimination. Care homes managers have pointed out that such reluctance or refusal to admit older care home residents to hospital could not be explained by need, as hospital bed capacity was never reached.’
‘The problem was widely reported early on in the pandemic, and was seemingly exacerbated by guidelines published by NHS England on its website on 10 April advising that some care home residents “should not ordinarily be conveyed to hospital unless authorised by a senior colleague.” The guidelines caused a controversy and were withdrawn a few days later but the damage lingered.’
‘Official figures show admissions to hospital for care home residents decreased substantially during the pandemic, with 11,800 fewer admissions during March and April compared to previous years.’
‘The son of one care home resident who passed away in Cumbria said that sending his father to hospital had not even been considered:
“From day one, the care home was categoric it was probably COVID and he would die of it and he would not be taken to hospital. He only had a cough at that stage. He was only 76 and was in great shape physically. He loved to go out and it would not have been a problem for him to go to hospital. The care home called me and said he had symptoms, a bit of a cough and that doctor had assessed him over mobile phone and he would not be taken to hospital. Then I spoke to the GP later that day and said he would not be taken to hospital but would be given morphine if in pain. Later he collapsed on the floor in the bathroom and the care home called the paramedic who established that he had no injury and put him back to bed and told the carers not to call them back for any Covid-related symptoms because they would not return. He died a week later.
“He was never tested. No doctor ever came to the care home. The GP assessed him over the phone. In an identical situation for someone living at home instead of in a care home, the advice was “go to hospital”. The death certificate says pneumonia and COVID, but pneumonia was never mentioned to us.”’
‘Reduced possibility to send care homes residents to hospital compounded another long-standing issue, that of care homes residents’ limited access to GPs. Obtaining access to GPs got markedly more challenging during the pandemic, as GPs throughout the country switched to phone/online consultations and stopped visiting care homes. NHS England advised GPs to begin the roll out of remote consultations on 17 March 2020, prioritising vulnerable groups but limiting face-to-face consultation to only “when absolutely necessary.” However, Amnesty International received multiple reports from care homes managers and staff and relatives of care home residents throughout the country of doctors refusing to enter care homes and only being available for consultations by phone or via video calls, no matter what the residents’ symptoms were and even in regard to end-of-life support.’
‘The daughter of a care home resident who died in Liverpool described the lack of medical care her father experienced:
“In the file it says that dad complained of chest pain on 28 March and asked to see a doctor but there was no follow up in the file … In the file it also says that dad had fallen on morning of 1 May and banged his head and had a swelling. I was never told and there is no record of a doctor being called for this. On 1 May a carer told me they had rang the doctor but the doctor was not going in [to the care home] and had prescribed antibiotic and end of life drugs. Then I spoke to the GP and he said he suspected COVID or chest infection and that I should go see him. Dad died on 2 May and a staff member told me she was there when dad died and he was gasping for breath and holding his chest.”’
It is self-evident that the withdrawal of medical care will cause excess deaths. It is also worthy of note that a GP was willing to prescribe end-of-life drugs over the telephone.
Misuse of ‘do not attempt resuscitation’ (DNAR) forms
Amnesty quote Parliament’s Joint Committee on Human Rights from September of 2020 as saying:
‘The blanket imposition of DNACPR notices without proper patient involvement is unlawful. The evidence suggests that the use of them in the context of the Covid-19 pandemic has been widespread.’
And go on to report that:
‘Care home managers reported to Amnesty International and to media cases of local GP surgeries or Clinical Commissioning Groups (CCGs) requesting them to insert DNAR forms into the files of residents as a blanket approach.
‘Asked about any blanket approaches to DNARs, one care home owner in the north of England told Amnesty International, “We had a letter to that effect from the practice. I refused to sign it and handle it like that.” Another reported that they were asked to insert DNAR forms into a number of residents’ files. A family from Lancashire told Amnesty International that their relatives had been asked to sign a DNAR form without having understood what it meant.
‘“The nurse from the GP surgery rang me up to say they decided mum is DNR. I asked why and she said “we did this across the home”, and I said “no, this should be done on individual cases and I don’t agree to it”. So I had it taken off … She also said that they would not take mum to hospital and again I said that is something that would have to be decided if and when need arose on the basis of the situation at the time. They had asked mum about the DNR and she had agreed to it but then I spoke to mum and she had not really understood the issue.”’’
Discharge of patients from hospitals into care homes
Amnesty reports that:
‘On 17 March 2020 NHS England announced the decision to urgently discharge patients, including those who were infected or who may have been infected with COVID-19, from hospitals into care homes and the community. This was among the most crucial decisions that adversely affected care homes across the country.’
‘According to the National Audit Office, this policy led to 25,000 people being sent untested from hospitals into care homes between 17 March and 25 April, putting at risk the health and indeed the lives of care home residents. The DHSC did not collect data on the extent to which care homes successfully isolated residents with confirmed or suspected COVID-19 and did not require local authorities to collect data either.’
‘The discharge of thousands of patients from hospitals to care homes in the days following 17 March was extremely rushed, leaving little or no time for consultations and assessments. “We had 500-600 empty beds and nobody coming into A & E so there really was no need for such rushed discharges,” a member of a discharge team at a hospital in the south of England told Amnesty International. A care home manager recalled: “Families learned their relatives came to care homes on the spot. There was no time for them to discuss with hospitals or with us. Families had no chance to choose which care home, to visit the place, to meet us. People’s teeth and glasses went missing in the rush.”’
In addition to infection risk, this also represents the denial of (presumably necessary) hospital care to thousands of elderly people—an action guaranteed to raise the death rate.
Increased workload, reduced staffing levels and removal of oversight for care homes
Compounding the medical problems, Amnesty’s report identified how COVID regulations reduced the number of staff, whilst increasing the workload of the remaining ones:
‘According to the National Audit Office, workforce shortage in the care sector pre-pandemic was already estimated at 122,000 and staff absence increased significantly during the pandemic, with absence rates in care homes between mid-April and mid-May 10% on average, and considerably higher in certain care homes or areas. The lack of testing exacerbated this problem as it was impossible to know if some of those self-isolating were COVID-19 free and could in fact work. Staff shortages in turn impacted the ability of care homes to adequately manage infections and the quality of care they were able to provide for residents, both those infected with COVID-19 and others. This was exacerbated by a situation where care home staff had to perform a number of additional tasks—from assisting residents to communicate with their relatives who could no longer visit them, to enforcing social distancing among residents unable to understand the requirement because of dementia, to cutting residents’ toenails because chiropodists stopped visiting care homes, to interpreting and communicating residents’ symptoms to GPs who were no longer visiting care homes, etc.’
This coincided with the removal of oversight from care homes, with the Care Quality Commission (CQC) suspending inspections and family members banned from visiting:
‘Beginning on 16 March 2020, the CQC announced that it would be ceasing its routine inspections of care homes, leaving open only the possibility of visits “in a very small number of cases when we have concerns of harm, such as allegations of abuse.” In its announcement, CQC said its primary objective was supporting providers “to keep people safe” and so there would be a “shift towards other, remote methods to give assurance of safety and quality of care.” Notably, this decision meant that at a time when older people in care homes were most vulnerable—because of the virus and because those who usually advocated on their behalf could no longer visit them—the regulator was largely absent.
‘The lack of official visits occurred at the same time as a ban on other visits—from family and friends, as well chiropodists, hairdressers, nurses, and others—which were normally an important source of information for the CQC. Expert noted that “[CQC] have been unable to rely on the ‘eyes and ears’ of visitors to raise the alarm and care workers have been frightened to speak out.”’
In other countries
Reports from the various countries experiencing high excess mortality at this time tell a similar tale. They were all engaged in isolating their elderly population and denying them medical care. In a report into the care home disaster in Sweden, the BBC quote a nurse as saying:
‘They told us that we shouldn't send anyone to the hospital, even if they may be 65 and have many years to live. We were told not to send them in.’22
In Spain, soldiers were brought into care homes and found residents dead in their beds, abandoned.23 In French homes, Reuters reported that ‘bodies have been left decomposing in bedrooms’.24 In Canada, the C2C Journal reported that:
‘Quebec’s Health Ministry issued a directive on March 19 – barely a week after the global pandemic had been declared – instructing nursing homes not to send residents to hospitals unless in exceptional circumstances. Conversely, hospital patients who were not in critical condition were to be either sent home or transferred to care homes. This practice was adopted in multiple jurisdictions: Quebec, Ontario, several U.S. States including New York and New Jersey, and in England.’25
New York Governor Andrew Cuomo’s order to nursing homes to admit COVID-19 patients was found by the State Bar Association to have increased the death toll among residents.26 New York also made extensive use of ventilators, which are estimated to have killed tens of thousands of Americans unnecessarily.27
End-of-life drugs
In 2020, British journalist Jacqui Deevoy began documenting stories of people who contended their family members had been effectively murdered by the NHS, through being involuntarily put on ‘end-of-life pathways’. This would be unbelievable, had it not already happened within the past decade, with the infamous Liverpool Care Pathway being phased out as recently as 2014.28
Ms. Deevoy placed particular emphasis on the sedative drug, midazolam. She documented family members’ accounts in her film, A Good Death?29 The documentary is a harrowing yet informative watch, where family members back their observations with data regarding the doses of midazolam being administered. They highlight a paradoxical effect, where the drugs given to treat an ailment actually produce the symptoms of that ailment, leading to the delivery of more drugs. The following quotations illustrate the families’ experiences:
‘Because they said “you can’t feed your wife”, as I was feeding her I was looking out the door. She said, “what do you keep looking at?” I said “I’m making sure the nurses aren’t coming in.”’
‘I’ve since found out that he was starved as well. His routine diet was discontinued three days before his death, with no water either.’
‘I think what happened was, because they neglected her, and they gave her a high dose of midazolam and morphine, because it is a respiratory suppressor, and they dehydrated her for such a long time, those drugs compounded and they were magnified in terms of potency, because she just couldn’t get the oxygen, she just suffocated.’
‘The last thing she said to me was: “get me out of this hospital, they’re trying to kill me.”’
‘What does it say on his death certificate that he died of?’
‘COVID-19 pneumonia'
‘And what do you think he died of?’
‘The midazolam.’
‘He was killed?’
‘Yes’
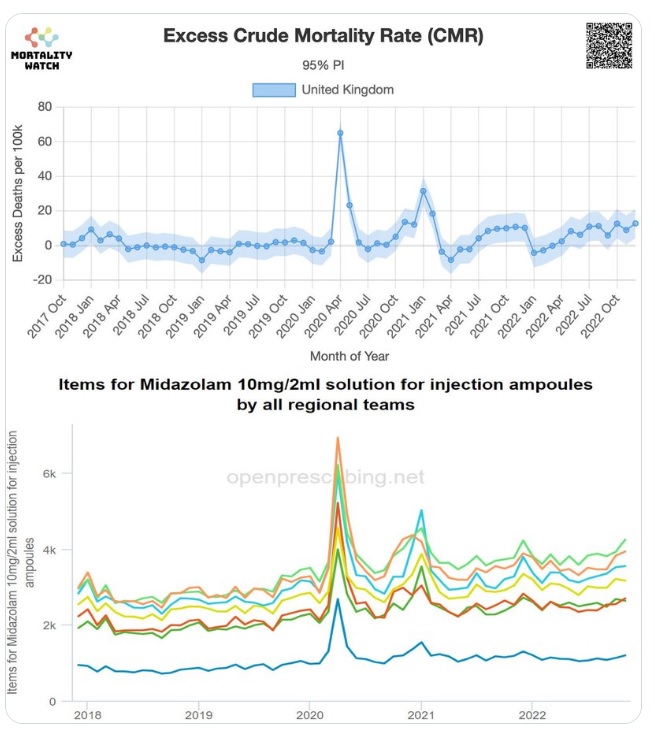
As we’ll see in a moment, midazolam use spiked in April of 2020. Was this because so many people were dying of COVID, or were people dying because of the increased use of a respiratory suppressant drug?
In a presentation titled Euthanasia in the Pandemic?30 Dr. John Campbell addressed this question by referring to the National Institute for Health and Care Excellence (NICE) COVID treatment guidelines, published on the 3rd of April 2020. The key line that jumps out in the Managing Breathlessness section is:
‘Sedation and opioid use should not be withheld because of an inappropriate fear of causing respiratory depression.’31
Dr. Campbell questions whether a fundamental mistake was made in transferring the guidelines for incurable conditions onto a potentially completely recoverable one. He points out that if an opioid and a benzodiazepine (such as morphine and midazolam, respectively) are given together, they will have the effect of stopping the recipient breathing. He states that:
‘Opioids and benzodiazepines will depress respiration. A lot of these people were breathless anyway, they had acute respiratory distress syndrome. If you have a lot of fluid in your alveoli you'll breathe more quickly to try and compensate and that can get enough oxygen into your body to mean that you survived the acute episode. But if you give these drugs, and you get respiratory depression, I don't think you need me to spell out the consequences of that. Not enough oxygen, tissue hypoxia, and death would be the result.’
Dr. Campbell goes on to say:
‘So they said “consider an opioid and a benzodiazepine like midazolam combination for patients with COVID-19 who are at the end-of-life.” But how many patients with COVID-19 would be at the end-of-life, unless they had some intractable condition at the same time? And how do you know if they're at the end-of-life? I've looked after hundreds of patients where I’ve thought “good grief they're not very well”, but the vast majority of them survive with an infectious condition. You can't really tell whether it's the end-of-life or not.’
And:
‘Even with moderate breathlessness people might have looked ill but had a virus that their immune system could have overcome. They could have recovered, but could well have been given these medications that resulted in suppressing their breathing.’
Serious concerns over the NICE guidelines were raised as early as the 20th of April 2020, in a letter to the British Medical Journal signed by two professors and nine doctors. They warned:
‘The combination of opioid, benzodiazepine and/or neuroleptic is used in specialist palliative care settings for symptom control and for ‘palliative sedation’ to reduce agitation at the end of life. It takes great skill and experience to use palliative sedation proportionately so that extreme physical and existential distress are palliated, but death is not primarily accelerated. NG163 states: “Sedation and opioid use should not be withheld because of a fear of causing respiratory depression.” If COVID-19 infection were uniformly fatal, this would be an acceptable statement. But for people not previously known to be at the end of life, there is potential risk of unintended serious harm, if these medications are used incorrectly and without the benefit of specialist palliative care advice.
‘Another concern is that the recommended doses for morphine and midazolam are sometimes higher than current guidelines state for non-specialist use; and moreover there are inconsistencies between the maximum doses recommended by the oral or subcutaneous routes.’32
Vastly increased use of midazolam is not only apparent, it corresponds with the increase in excess mortality seen in 2020:33
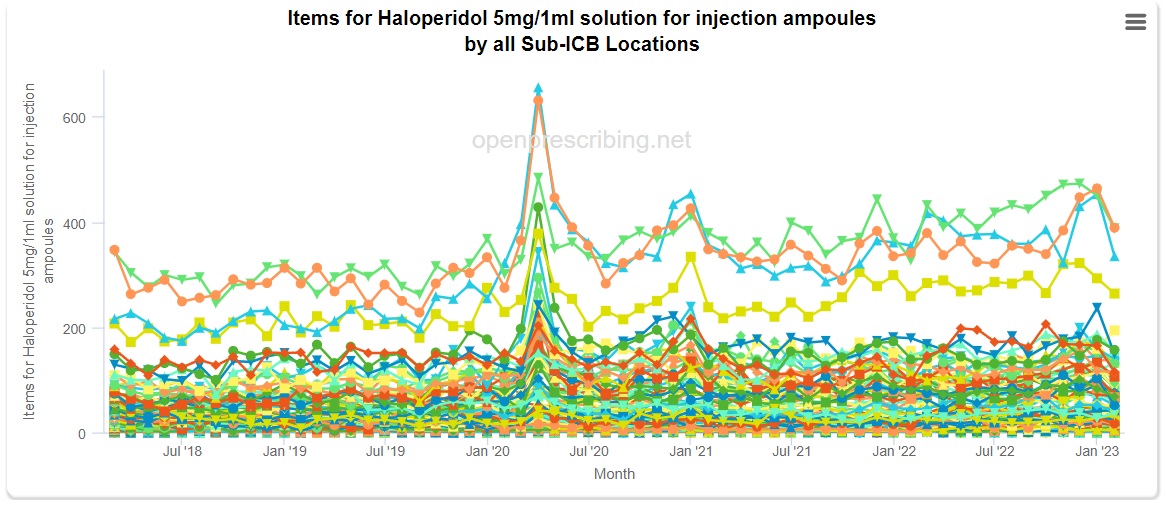
Dr. Campbell goes on to demonstrate a similar spike in prescriptions for the drugs levomepromazine and haloperidol, the latter of which is not approved for use in older adults due to ‘risk of death’.34
There is also evidence for increased midazolam use in Italy and Sweden.35 Israel National News reported comments from Swedish Professor of Geriatric Medicine, Yngve Gustafson:
‘“Living in a nursing home is not a diagnosis. By itself it can never be a medical basis for deciding whether to live or die”. Gustafson said that nutrient drip treatment, blood clot prevention, oxygen and bacterial pneumonia treatment with antibiotics would help the elderly. “Instead, giving morphine and midazolam regularly to elderly people with lung infection is active euthanasia, if not something worse. We gave up the elderly who could have had a chance of survival”.’36
Decrease in antibiotics prescriptions
In 2008 none other than Dr. Anthony Fauci himself co-authored a paper on postmortem studies of victims of the pandemic of 1918. The paper found that:
‘People who died of influenza during 1918–1919 uniformly exhibited severe changes indicative of bacterial pneumonia. Bacteriologic and histopathologic results from published autopsy series clearly and consistently implicated secondary bacterial pneumonia caused by common upper respiratory-tract bacteria in most influenza fatalities.’
And concluded that:
‘The majority of deaths in the 1918–1919 influenza pandemic likely resulted directly from secondary bacterial pneumonia caused by common upper respiratory-tract bacteria. Less substantial data from the subsequent 1957 and 1968 pandemics are consistent with these findings. If severe pandemic influenza is largely a problem of viral-bacterial copathogenesis, pandemic planning needs to go beyond addressing the viral cause alone (e.g., influenza vaccines and antiviral drugs). Prevention, diagnosis, prophylaxis, and treatment of secondary bacterial pneumonia, as well as stockpiling of antibiotics and bacterial vaccines, should also be high priorities for pandemic planning.’37
Given this, in combination with Dr. Fauci’s prominent role during the pandemic, it is surprising that we haven't heard more about the dangers of secondary bacterial infections over the past three years. What role have they played in COVID-19 deaths?
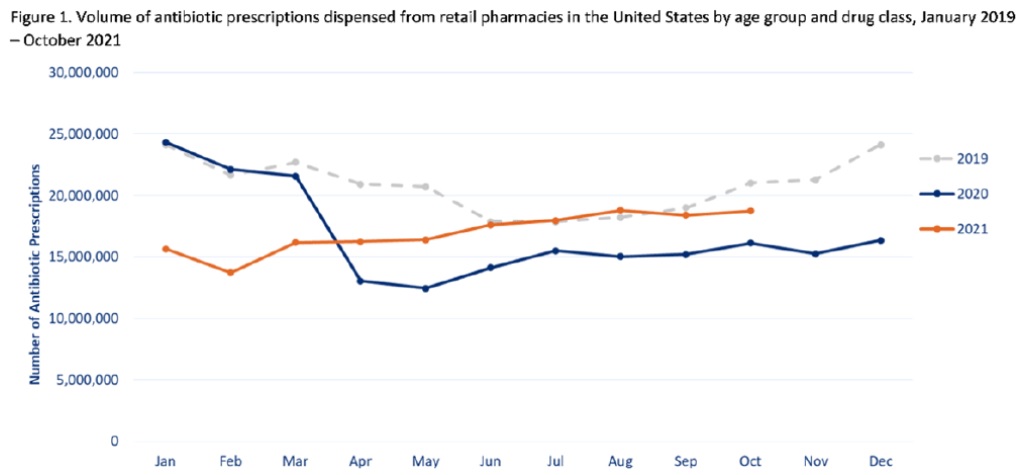
In actual fact it is no secret that prescriptions for antibiotics fell dramatically through the COVID era, once again in a manner that correlated with rising excess mortality:38
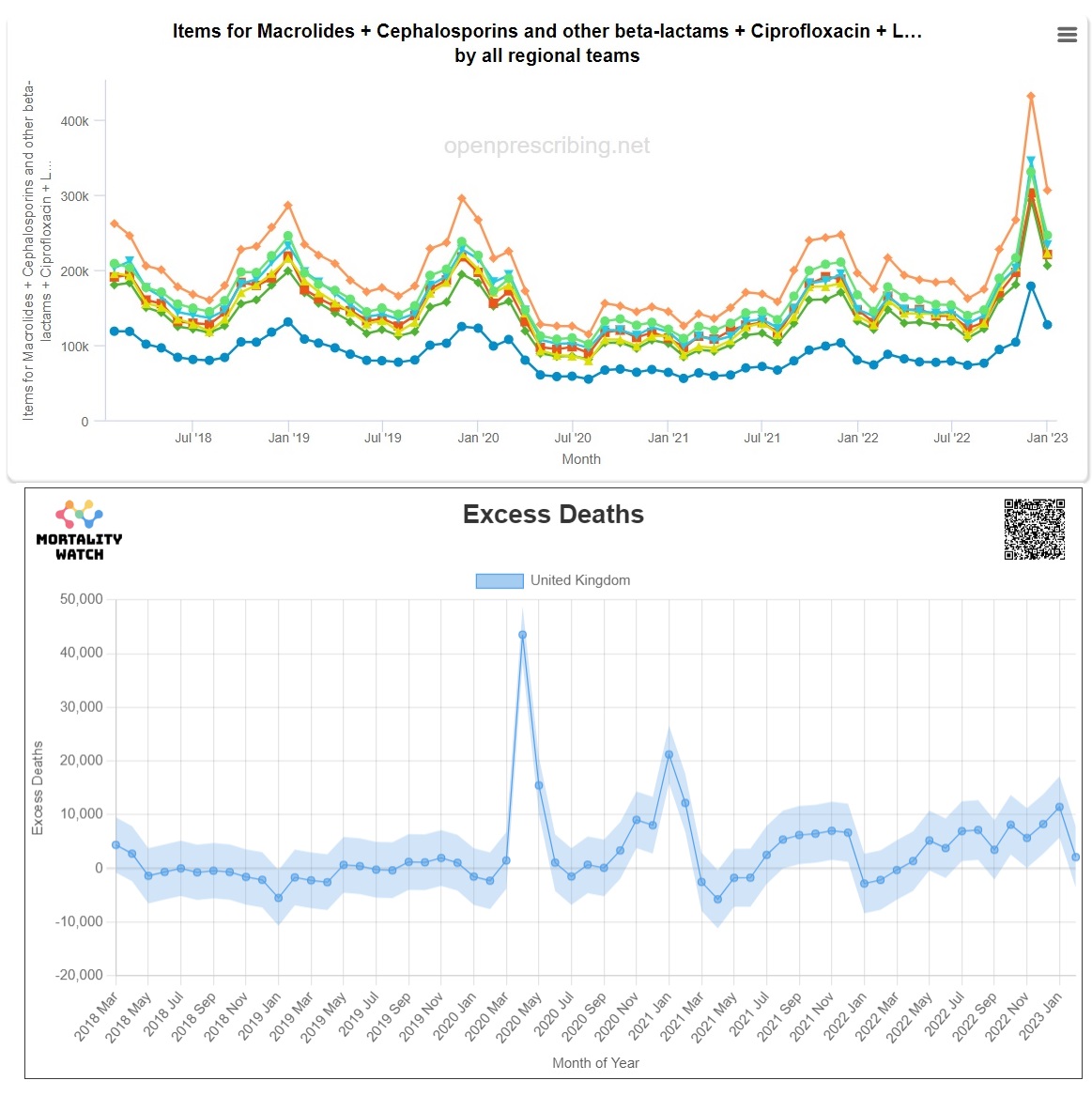
Antibiotic rates in March of 2020 are comparable with the previous two years. Prescription rates decrease in April, then remain low until 2022. The previous winter spike is simply not present in January of 2021, at exactly the time an unusual spike arises in excess mortality.
A similar situation is observable in the USA:39
This data led Dr. Denis Rancourt to propose:
‘It is not unreasonable to ask whether the logic has not been inverted: Is COVID-19-assignment an incorrect cause-assignment for what is in fact bacterial pneumonia?’
‘If COVID-19 is largely misdiagnosed bacterial pneumonia (using a faulty PCR test: Borger et al., 2021; or not using any laboratory test), or if co-infection with bacterial pneumonia is not appropriately recognized (Ginsburg and Klugman, 2020), or if bacterial pneumonia itself goes otherwise untreated, while antibiotics (and Ivermectin) are withdrawn, in circumstances where large populations of vulnerable and susceptible residents have suppressed immune systems from chronic psychological stress induced by large-scale socio-economic disruption, then the state has recreated the conditions that produced the horrendous bacterial pneumonia epidemic of 1918 (Morens et al., 2008) (Chien et al., 2009) (Sheng et al., 2011), in COVID-era USA.’40
Conclusion
The aim of this chapter has not been to demonstrate what caused the increase in excess mortality over the past several years. Instead, it has been to identify that multiple factors have been at play, and it is not easy (perhaps impossible) to point to one of them as causal.
Perhaps Claus Köhnlein and Torsten Engelbrecht will ultimately be proven correct, that all excess deaths were iatrogenic. Maybe Denis Rancourt’s view that a virus was involved, but not necessarily a novel one, will win out. Maybe the deaths are a split between a novel coronavirus and iatrogenic factors. It is certainly far beyond the scope of this document to come down on any side of a line.
What is well within scope, is to propose that this question—the question of what caused the excess deaths—is undoubtedly one of the most important in the world right now. Without answering it, societies around the globe will be doomed to repeat the devastating mistakes of the COVID era.
Supplemental: an account from a nursing home manager on the Isle of Man
Amnesty International’s report, As If Expendable, highlighted the difficulty nursing homes faced maintaining staffing levels due to stringent isolation requirements. This situation led to a staffing crisis at Abbotswood Nursing Home on the Isle of Man. The result of this was that the Island’s Department of Health and Social Care (DHSC) suspended the home’s licence and took direct control. We are not aware of this happening anywhere else in the British Isles. Prior to this, two residents had died (both discharged from hospital on end of life care). After the takeover, fourteen residents died within two weeks. A further four died after this.
Mrs. Zandra Lewis was a registered nurse and a Director and responsible person of Abbotswood at the time the COVID-19 pandemic was announced. She had held a managerial position there since 1994. Mrs. Lewis strongly disputes that there was any reason for the DHSC to take the unprecedented course of action it embarked on. She further contends that the deaths at Abbotswood that occurred after the DHSC took over were essentially iatrogenic: brought about by residents being placed on ‘end-of-life’ pathways. In a letter delivered to the Island’s Chief Constable in June of 2020, Mrs. Lewis asserted that the DHSC:
Failed to provide basic medical care such as subcutaneous drips or oxygen to try and save residents' lives.
Failed to identify and treat residents' illnesses and medical issues and provide adequate care.
Refused to transfer ill residents to Nobles hospital, where appropriate medical care in a hospital setting may have changed their ultimate outcome.
Failed to provide appropriate hygiene care to residents, mouth care, grooming and washing.
Failed to feed and provide fluids to residents resulting in weight loss and dehydration (staff remaining at Abbotswood informed Mrs. Lewis that they were taken away from essential care such as giving fluids and feeding residents to change pads).
Used lethal end-of-life drugs such as midazolam and morphine.
This list is by no means exhaustive. It parallels issues raised in the Amnesty report. A criminal investigation was launched into the directors of the home, however no criminal charges were brought.41 In spite of the deaths happening on their watch, no investigation into the actions of the DHSC has ever been held.
In a statement submitted to the Island’s Independent COVID Inquiry, Mrs. Lewis recounted the toll this had taken on her:
‘I was so distressed by what the DHSC, hounding, bombardment, intolerable way that my residents, their families, staff of Abbotswood, managers and directors had been treated, I could no longer tolerate this, they had physically and emotionally set out to break me, they had managed to rip my heart and soul out of everything I loved and stood for. I had always put my residents first over anything else. They were my family and we all at Abbotswood had nursed and nurtured them to an extremely high standard. I couldn’t take this torture any longer, I was depressed by everything and extremely distressed at the DHSC disregard, lack of compassion, respect, or tolerance. As one of the first homes to get Covid, we were still in the learning stages of the disease, as we still are, we were set upon and held up as an example. We had no right of reply, they used the media to their own advantage, and we were not allowed to say anything. They ruined us, acted unethically, and drove me to try and take my own life, by walking into the sea. I was brought out by two people I did not know. They knew I was unwell but continued to bombard me. I thus went on to have a heart attack and was flown over to Liverpool.’
Finally, Mrs. Lewis described an incident, relayed to her by Abbotswood staff, as an example of how residents were treated:
‘The most horrific thing was the last resident to leave the building was in the last throes of end of life care. The Abbotswood staff who were left asked the DHSC staff to let her stay and they would look after her so she could have a peaceful end. They said No and moved her. She died as she reached the hospital.’42
Questions for the State
Can the state offer reassurance that deaths attributed to COVID-19 were not in fact iatrogenic? This would include but not be limited to:
Use of drugs such as midazolam, morphine and haloperidol etc.
Decreased prescriptions of antibiotics
Refusal to provide medical services to any people, either by restricting hospital visits or access to GPs
Use of ‘end-of-life’ pathways, involving withdrawal of medical care, food and water etc.
Use of ventilators
Did the state experience increased use of drugs such as midazolam, or a decrease in antibiotic prescriptions during the pandemic period?
Given the evidence presented in this chapter, what conclusions does the state now draw about the international excess mortality which influenced policy?
Would state policy have been different if the iatrogenic hypothesis had been considered/known?
How will the state take the apparent ambiguity inherent in spikes in all cause mortality into account in the event of a future pandemic being announced?
Two. Mask Mandates
Anthony Fauci: ‘Right now in the United States, people should not be walking around with masks. When you're in the middle of an outbreak wearing a mask might make people feel a little bit better, and it might even block a droplet, but it's not providing the perfect protection that people think that it is and often there are unintended consequences. People keep fiddling with the mask and they keep touching their face.’
Interviewer: ‘And can you get some sort of smutz staying inside there?’
Anthony Fauci: ‘Of course, of course.’1
When compared to the controversies of excess deaths, accusations of manslaughter, life changing vaccine injuries and the inhumanity of lockdowns, the issue of mask mandates may seem like a relative triviality. If they helped ‘stop the spread’ then great, and if not—what did we really lose by trying?
The deeper question raised by mandates however, is at what point is it acceptable for one group of people to impose medical interventions upon others? Is it after a certain amount of scientific evidence of efficacy has accumulated? Is it when a certain level of popular consent is attained? Can it only be done after a thorough study of potential harms? And what about the very nature of mandates, to what extent do any unintended and adverse effects of mandating behaviour need to be taken into account?
This raises the further question: if mandates turn out to have a counterproductive or even harmful effect, what sanction should fall upon those who imposed them?
Mask mandate efficacy
As the opening quotation of Dr. Anthony Fauci illustrates, at the start of the COVID era, masks were not generally regarded as helpful in preventing the spread of viruses.2 This is reflected in mask literature up until 2020. As an example from the New England Journal of Medicine:
‘We know that wearing a mask outside health care facilities offers little, if any, protection from infection…In many cases, the desire for wide spread masking is a reflexive reaction to anxiety over the pandemic.’3
And the Centers for Disease Control (CDC):
‘We did not find evidence that surgical-type face masks are effective in reducing laboratory-confirmed influenza transmission, either when worn by infected persons (source control) or by persons in the general community to reduce their susceptibility.’4
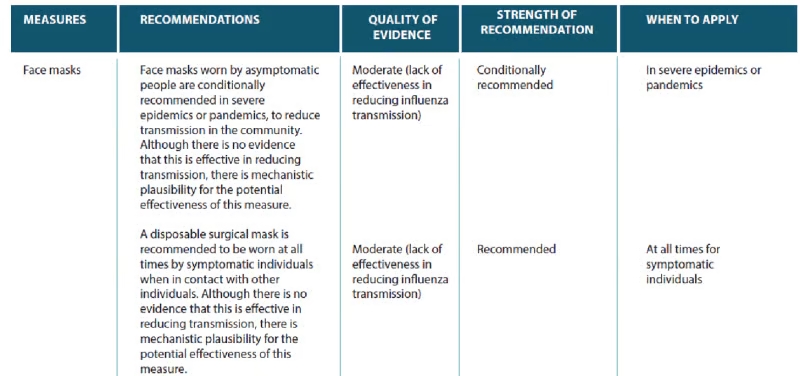
The World Health Organisation’s pandemic planning document from 2020 acknowledged that there was ‘no evidence’ that face masks were effective at reducing transmission in the community. The WHO ‘conditionally recommended’ masks, on the basis of a ‘mechanistic plausibility’ for ‘potential’ effectiveness.5
Indeed, in March 2020 US Surgeon General Dr. Jerome Adams even went so far as to say masks might actually increase the likelihood of infection.6
By May, a turn of opinion emerged. A paper published in The Lancet acknowledged the absence of evidence for masking, but claiming this did not amount to evidence of absence:
‘However, there is an essential distinction between absence of evidence and evidence of absence. Evidence that face masks can provide effective protection against respiratory infections in the community is scarce, as acknowledged in recommendations from the UK and Germany. However, face masks are widely used by medical workers as part of droplet precautions when caring for patients with respiratory infections. It would be reasonable to suggest vulnerable individuals avoid crowded areas and use surgical face masks rationally when exposed to high-risk areas. As evidence suggests, COVID-19 could be transmitted before symptom onset, community transmission might be reduced if everyone, including people who have been infected by an asymptomatic and contagious, wear face masks.’7
By September, the New England Journal of Medicine reported that:
‘As SARS-CoV-2 continues its global spread, it’s possible that one of the pillars of Covid-19 pandemic control — universal facial masking — might help reduce the severity of disease and ensure that a greater proportion of new infections are asymptomatic. If this hypothesis is borne out, universal masking could become a form of “variolation” that would generate immunity and thereby slow the spread of the virus in the United States and elsewhere, as we await a vaccine.’8
At this time, CDC director Robert Redfield became so confident in masking he stated that:
‘I might even go so far as to say that this face mask is more guaranteed to protect me against COVID than when I take a COVID vaccine’.9
It’s fair to say that the issue of masking transcended science and became politicised. This politicisation was exasperated by the especially contentious US election of 2020.10
Over the following months a number of studies were published, which concluded both for and against masking.11 The former category was of course employed to justify mask mandates. Some in this category looked only at the mechanical plausibility of masks, whilst others were substantially critiqued for containing obvious methodological flaws.12
Two of the most prominent were conducted in Denmark and Bangladesh. The DANMASK-19 study, published in March of 2021, found no personal protective effect from masking.13 It was critiqued for setting too high a bar for success.14
The Bangladesh study showed no benefit from cloth masking (the only kind that was ever mandated), but found surgical masks lowered rates of COVID-19 by 11.2%.15 This study was critiqued for significant bias.16
The most definitive review of mask efficacy (due to it being a meta study) must be the Cochrane Database’s Physical interventions to interrupt or reduce the spread of acute respiratory viruses, published in January of 2023. The review concluded that:
‘The pooled results of RCTs did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks. There were no clear differences between the use of medical/surgical masks compared with N95/P2 respirators in healthcare workers when used in routine care to reduce respiratory viral infection.’17
Lead author, Dr. Tom Jefferson, commented that:
‘Governments had bad advisors from the very beginning… They were convinced by non-randomised studies, flawed observational studies. A lot of it had to do with appearing as if they were “doing something.” ‘18
And:
‘There’s no evidence that masks work. It’s possible they could work in some settings….we’d know if we’d done trials. All you needed was for Tedros [from WHO] to declare it’s a pandemic and they could have randomised half of the United Kingdom, or half of Italy, to masks and the other half to no masks. But they didn’t. Instead, they ran around like headless chickens.’19
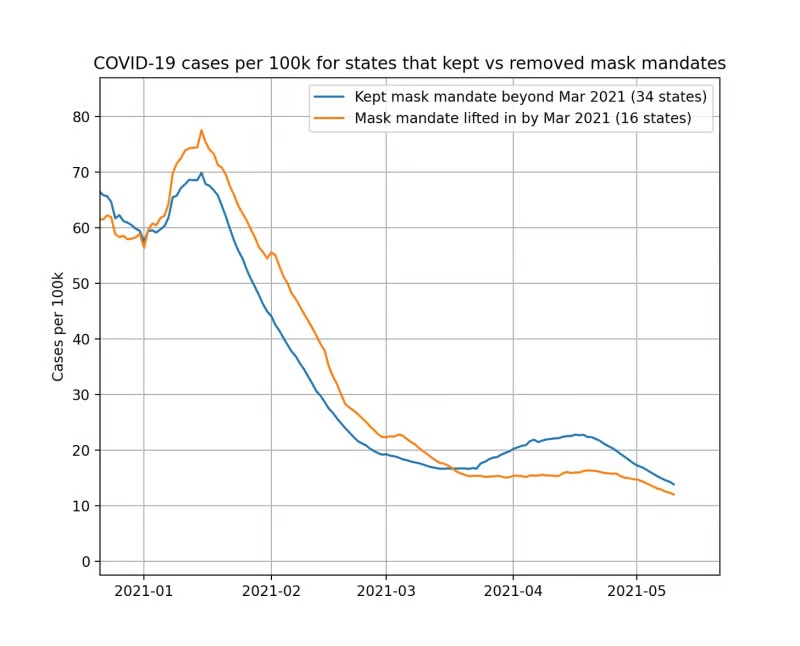
Whilst it is true that some epidemiologists contend Dr. Campbell draws too critical a conclusion from his data20 (an accusation he certainly does not accept), even if this is allowed, the evidence for masking is at best weak and in greater likelihood, nonexistent. This would explain why the effects of mask mandates are consistently invisible in real world comparisons.21
The debate is really not just about whether masks can be shown to work at all or not—if a person chooses to wear one in spite of the lack of evidence that’s their business—but what level of evidence would be required to mandate masks, and has that level been reached?
A thought experiment might be instructive: would any of the evidence for masking convince you that it is okay to engage in a behaviour whilst wearing a mask, that you wouldn’t engage in otherwise? The universal answer is ‘no’. If you cannot stand closer to someone masked than unmasked, shouldn’t you stand further away when unmasked? This is really the acid test, as if people truly believed masking worked, they would set different risk levels whilst wearing them. The fact that behaviours are recommended to remain the same masked and unmasked flies in the face of this.
Mask mandate harms
In April of 2020 the British Medical Journal published a letter from epidemiologist Dr. Antonio Lazzarino; regarding the mandating of masks he cautioned:
‘The precautionary principle aims at preventing researchers and policy makers from neglecting potentially-harmful side effects of interventions. Before implementing clinical and public health interventions, one must actively hypothesise and describe potential side effects and only then decide whether they are worth being quantified on not.’22
It would of course be no good thing if masks were ineffective, however if that were the limit of it, it could perhaps be argued that this isn’t too bad. We wasted some money on an ineffective preventative measure. If mask mandates are actively harmful however, this would of course be far worse.23
Serious concerns over the ‘potentially-harmful side effects’ of mask mandates have taken the following forms:
Masks restrict breathing and increase levels of carbon dioxide
A letter to the Belgian authorities, signed (at the time of writing) by 762 medical doctors and a further 2,931 medically trained health professionals, stated that:
‘Wearing a mask is not without side effects. Oxygen deficiency (headache, nausea, fatigue, loss of concentration) occurs fairly quickly, an effect similar to altitude sickness. Every day we now see patients complaining of headaches, sinus problems, respiratory problems and hyperventilation due to wearing masks. In addition, the accumulated CO2 leads to a toxic acidification of the organism which affects our immunity.’24
The Belgian doctors are not restricted just to their observations in support of these claims, several studies have observed how masks adversely affect breathing and the knock on health effects. This has been of particular concern with regard to the performance of surgeons.25
The direct relevance of this is that numerous studies have demonstrated a link between hypoxia (low oxygen blood levels) and suppression of the immune system. This is not to mention cancer and heart disease.26 Even if masks do keep viruses out (or in), then how should this be balanced against plausible immune system suppression?
It must be acknowledged that not all mask studies have found breathing impairment,27 but the precautionary principle demands that the studies that have are given consideration. A recent meta study concluded:
‘This systematic review comprehensively revealed ample evidence for multiple adverse physio-metabolic and clinical outcomes of medical face masks, with worse outcomes in the case of N95 masks. This can have long-term clinical consequences, especially for vulnerable groups e.g., children, pregnant, older adult, and the ill. Besides transient and progressive hypoxemia, hypercarbia, and individualized clinical symptoms our findings are in line with reports on face masks caused down-stream aberrations (e.g., oxidative stress, hypercapnia, vasoconstriction, pro-inflammatory response, immunosuppression etc.) at the organ, cellular and microbiome levels and support the MIES (Mask Induced Exhaustion Syndrome). From our point of view, while a short application of the mask seems to be less harmful, longer and long-term use may cause a shift toward the pathophysiological direction with clinical consequences even without exceeding physiological thresholds (O2 and CO2).’
And goes on to say that:
‘So far, several MIES symptoms may have been misinterpreted as long COVID-19 symptoms.’28
Masks are a breeding ground for bacteria
However credible the idea that breathing behind a barrier may guard against viral transmission may be, surely the idea that placing a damp and dirty rag in front of one's breathing apparatus could cause harm, is at least equally plausible. In recognition of this fact, the Journal of the American Medical Association (JAMA) advises:
‘Before putting on a face mask, wash your hands with soap and water for at least 20 seconds or use an alcohol-based hand sanitizer (with at least 60% alcohol). Without touching the front of the mask, secure the ties behind your ears or head. While wearing the mask, do not touch the mask or your face. When removing the mask, take off the ear loops or ties first. Do not touch the front of the mask or your face when removing the mask. After removing the mask wash your hands with soap and water for at least 20 seconds (or use hand sanitizer). Face masks should be washed routinely with soap and water or laundry detergent to prevent contamination.’29
It is perhaps self-evident that the vast majority of the general public were not adhering to such standards over a prolonged time period—neither could they realistically be expected to.
Various studies have confirmed the self-evident presence of bacteria on masks.30
A group of parents in Florida became so concerned about the effects of wearing masks (visible in the picture below) they sent six to the University of Florida for analysis. The resulting report found that five masks were contaminated with bacteria, parasites, and fungi, including three with dangerous pathogenic and pneumonia-causing bacteria.

Whilst there is obviously no chain of custody with these masks, it is a testimony to what concerned citizens can do, and is confirmed by findings.31
Besides it being common sense that it is not good to inhale bacteria, the role of bacteria in pandemics is not reckoned to be small. The 2008 paper, co-authored by Dr. Anthony Fauci, discussing the role of secondary bacterial pneumonia in the Spanish Flu, was discussed in Chapter One. It is worth requoting here:
‘People who died of influenza during 1918–1919 uniformly exhibited severe changes indicative of bacterial pneumonia. Bacteriologic and histopathologic results from published autopsy series clearly and consistently implicated secondary bacterial pneumonia caused by common upper respiratory-tract bacteria in most influenza fatalities.’
It concluded that:
‘The majority of deaths in the 1918–1919 influenza pandemic likely resulted directly from secondary bacterial pneumonia caused by common upper respiratory-tract bacteria. Less substantial data from the subsequent 1957 and 1968 pandemics are consistent with these findings. If severe pandemic influenza is largely a problem of viral-bacterial co-pathogenesis, pandemic planning needs to go beyond addressing the viral cause alone (e.g., influenza vaccines and antiviral drugs). Prevention, diagnosis, prophylaxis, and treatment of secondary bacterial pneumonia, as well as stockpiling of antibiotics and bacterial vaccines, should also be high priorities for pandemic planning.’32
Given Dr. Fauci's involvement with this study, it is surprising he has not mentioned it during his transition from mask cynic to advocate.
Masks and all cause mortality
By comparing mortality rates in Kansas counties with and without mask mandates, Dr. Zacharias Fögen studied whether masks decrease or increase all-cause-mortality. He concluded that:
‘Results from this study strongly suggest that mask mandates actually caused about 1.5 times the number of deaths or ∼50% more deaths compared to no mask mandates. This means that the risk for the individual wearing the mask should even be higher, because there is an unknown number of people in Mask Mandate Counties who either do not obey mask mandates, are exempted for medical reasons or do not go to public places where mask mandates are in effect. These people do not have an increased risk and thus the risk on the other people under a mask mandate is actually higher.’33
Masks cause viruses to be re-inhaled
Dr. Fögen contends that the vast majority of these excess deaths were due to re-inhalation of the COVID-19 virus, in what he termed the Foegen effect:
‘The fundamentals of this effect are easily demonstrated when wearing a facemask and glasses at the same time by pulling the upper edge of the mask over the lower edge of the glasses. Droplets appear on the mask when breathing out and disappear when breathing in.
‘In the “Foegen effect,” the virions spread (because of their smaller size) deeper into the respiratory tract. They bypass the bronchi and are inhaled deep into the alveoli, where they can cause pneumonia instead of bronchitis, which would be typical of a virus infection. Furthermore, these virions bypass the multilayer squamous epithelial wall that they cannot pass into in vitro and most likely cannot pass into in vivo. Therefore, the only probable way for the virions to enter the blood vessels is through the alveoli.
‘Moreover, the “Foegen effect” could increase the overall viral load because virions that should have been removed from the respiratory tract are returned.’34
Masks are composed of chemicals which can be toxic
In 2021 Health Canada advised Canadians not to use disposable face masks that contain graphene. This warning came after masks containing potentially toxic material were distributed to schools and healthcare facilities. Daycare educators became suspicious of the masks due to feeling like they were ‘swallowing cat hair’ while wearing them.35
It appears the science on the safety of the mask itself is minimal. One paper indicates the presence of potential toxic titanium dioxide in masks, whilst another looked at microplastic inhalation and considered it to be minimal.36
Microplastics are certainly a problem for the environment, where they have been described as ‘an environmental disaster that might last generations’.37
Mask mandates and risk compensation
It has not been uncommon to hear proponents of mask mandates compare them to seatbelt mandates: controversial and resisted when introduced, but now overwhelmingly accepted as being in everyone’s best interest. The comparison is not without irony, as seatbelt laws are often used to explain the difficulty of mandating for safety and the concept of Risk Compensation.
Risk Compensation suggests that people have a certain level of risk they find acceptable, and when safety measures are mandated they will simply increase risky behaviour to keep that level constant. It was originally studied when the introduction of mandatory seat belt laws across the United States did not seem to deliver the expected drop in traffic fatalities. It appears people wearing seatbelts feel safer and therefore will drive slightly faster. It can be easier to understand this the other way round, imagine how you might slow down and drive more carefully if you took your seatbelt off.38
Whether compensatory behaviours erase the benefits of safety mandates or not is a hotly contested issue. It has been particularly so during the COVID-19 era, with some claiming that the concept of Risk Compensation is overblown and has led to health authorities being too reticent to introduce mandates.39
Critics overwhelmingly agree however, that there is some offsetting effect to safety regulations. The debate is in regard to how much.40 Those who advocate mask mandates in spite of Risk Compensation, do so under the assumption that masks are substantially effective at preventing viral spread. If this is not the case, or if the prevention is trivial, then masks can only act to increase ‘risky’ behaviour.41
If the iatrogenic hypothesis discussed in Chapter One is correct, then this is irrelevant, as there is no ‘risk’ to increase. By the standards of governments who mandated masks however, this is not the case: there is serious risk posed by a deadly virus. In the absence of evidence for efficacy, we would have to conclude masks had not a neutral—but a harmful effect.
Conclusion
Whilst other issues with masks, such as their effects on childhood development and the publication of previously private medical information are of course major issues too,42 this chapter has sought to question whether masks can be justified even in terms of their stated goals. Irrespective of any other downsides, do they actually improve physical health?
Even ignoring health harms, It is clear that the evidence for this is weak at best and more likely: none existent. If we include the potential harms, the risks can not possibly be said to outweigh the negative consequences. Furthermore, it is not just a case of demonstrating a small effect, but of demonstrating a large and safe enough one to justify imposing masks on unwilling wearers. This condition has clearly not been met.
Questions for the State
What scientific evidence did the state rely on to justify the imposition of mask mandates?
How was the state able to dismiss evidence (such as the Cochrane Review from 2020) that masks were ineffective?
How did the state consider the precautionary principle when both ‘expecting’ and mandating masks?
What is the state’s response to the potential harms from mask wearing identified in this document?
Is the state taking any action to observe if mask mandates caused health problems in the population?
Given the recent publication of the updated Cochrane Review, and the problems with mask studies highlighted in this paper, what is the state’s current position on the efficacy and safety of masks?
Did the state consider risk compensation when mandating masks? If so, how did the state conclude that the apparent benefits of masks would outweigh risk compensating behaviour?
Three. Lockdowns
‘Deaths Soar In Country That Didn’t Lock Down.’
CNN Headline, 29th April, 20201
The dawning of a new decade may bring with it a sense of optimism. For our current one, there was something exciting about living in the twenties, with its historic connotations of social liberation and celebration. If at a New Year’s Eve party, someone had prophesied that the majority of the world’s liberal democracies would soon be imposing business closures and a form of house arrest on their citizens, they would have appeared quite mad.
The ‘roaring’ 1920s took over nine years to crash. Ours did so within three months.
The consequences of lockdowns were as brutal as they were predictable.2 The United Nations warned of ‘multiple famines of biblical proportions’, that would kill ‘hundreds of thousands of children’,3 whilst Oxfam cautioned that ‘the economic crisis is potentially going to be even more severe than the health crisis’, moving half a billion people into poverty.4 The inevitable rise in child trafficking was not long in coming.5 Commenting on cutbacks in essential medical care; the BBC speculated that ‘most COVID-19 deaths won’t be from the virus’.6 The Daily Mail reported that hundreds of cancers were being missed each week because screening had been suspended.7
The implications of isolation for the elderly scarcely need pointing out, yet it is worth doing so anyway. To quote from Amnesty International’s report on the UK Government's abuse of the elderly once more:
‘After not seeing mum for months I found her terribly weakened, both physically and mentally. We were sitting in the garden several metres apart and she was crying all the time. Communicating at a distance is exhausting for her as she can’t hear properly. Mum doesn’t have dementia and before Covid used to have a lot of visitors, friends who live nearby visited every day. Now she has lost the will to live.’
And:
‘For five and a half months I only had window visits and during the last window visit I touched my mum’s hand through the small window opening, having first used hand sanitizer. I did so because mum was in pain and was crying. A carer saw this and my mum was put in isolation for two weeks. My mum already had COVID two months earlier and both my mum and I tested negative two days after the incident, but despite this she was still kept in isolation for the full two weeks. This is unnecessary and cruel. Before lockdown my mum was mobile and I used to take her out often, but since lockdown she has been kept in a wheelchair and has deteriorated sharply. Yesterday I had the first garden visit and for the first time she could no longer have a conversation.’8
What could justify the implementation of a policy guaranteed to cause millions of deaths, decimate the global economy and deprive people of all quality in their lives? Surely the precautionary principle would demand overwhelming evidence that the policy would save substantially more lives than it destroyed? What was the historical precedent for this?
Even if the pessimistic New Year’s reveller mentioned above had been a student of pandemic preparedness, it’s unlikely he would have been able to predict lockdowns. World Health Organization public health measure advice as of 2019 recommends the voluntary isolation of sick individuals in their homes. Even in doing so, it acknowledges this poses an increased risk of infection to those cohabiting, and that ‘older adults who live alone may not receive sufficient care and support when home isolation is implemented’. The report further acknowledges that the effectiveness of isolation is ‘moderate’, and that the quality of evidence supporting it is ‘very low’. The duration of isolation is reckoned to be between five and seven days.
The quarantining of exposed individuals is not recommended, due to ethical considerations, a very low quality of evidence and ‘no obvious rationale for this measure.’ The mandatory quarantining of an entire population of healthy individuals is not even considered.
School and workplace closures and avoiding crowds are all ‘conditionally recommended’ in extreme circumstances. This semi-recommendation comes with the caveat that these interventions obviously bring their own harms, and that there is ‘very low’ overall quality of evidence that they reduce transmission.
International travel restrictions are conditionally recommended ‘during the early stage of a localised extraordinarily severe pandemic for a limited period of time’, with the same caveats as above. Full border closures are not recommended, due to ‘very low quality of evidence, economic consequences, resource implications and ethical implications.’9
These were the positions of the WHO when the Chinese Communist Party (CCP) alerted them to an outbreak of viral pneumonia on the 31st of December, 2019.
On the 23rd of January, the CCP ordered a lockdown of fifty eight million people in Hubei province. At this point a total of eighteen people had been classified as dying of COVID-19 in Wuhan. Wuhan has a population of around nine million and is known as Smog City.10 The CCP had violently suppressed protests there over air pollution,11 which does not seem to have been considered a factor in these deaths.12
At this time, strange videos emerged of people purportedly from Wuhan dropping dead in the streets. Whether these were deliberate propaganda or just the internet doing its thing is unknown, but they had the effect of terrifying the world.13
At this time, there was still no indication that Western health authorities favoured lockdowns, with Anthony Fauci commenting on the 28th of February:
‘That’s something that I don’t think we could possibly do in the United States, I can’t imagine shutting down New York or Los Angeles, but the judgement on the part of the Chinese health authorities is that given the fact that it’s spreading throughout the provinces... it’s their judgement that this is something that in fact is going to help in containing it. Whether or not it does or does not is really open to question because historically when you shut things down it doesn’t have a major effect.’14
The WHO acknowledged the uniqueness of the CCP approach, saying:
‘It has not been tried before as a public health measure, so we cannot at this stage say it will or will not work….The lockdown of 11 million people is unprecedented in public health history, so it is certainly not a recommendation the WHO has made.’15
On the 30th of January Italy’s Prime Minister, Giuseppe Conte, declared a six month state of emergency after two Chinese tourists from Wuhan fell ill and tested positive for COVID-19. Conte was president of Italy’s Five Star Movement (M5S), which for the previous two years had sought closer economic ties to China.16
Perhaps strangely, these closer ties involved healthcare. A Plan of Action on Health Cooperation between the two countries had been signed in March of 2019, and further updated in November.17 This included cooperation in the ‘prevention of infectious diseases.’ This was a continuation of health cooperation plans between Italy and China first launched in the year 2000, by former Prime Minister Massimo D’Alema, a one time member of Italy’s Communist Party.18 It is worth mentioning that D’Alema now serves as honorary president of the Silk Road Cities Alliance, a Chinese state organisation.19
On the 22nd of February, fifteen cases of COVID were detected, and a fifteen day lockdown was implemented in the northern provinces of Lombardy and Veneto to ‘slow the spread.’20 This was on the basis of the deaths of seven people, the overwhelming majority of whom were elderly people who had also been suffering from other health issues.21 To put that in context; an average February in Italy sees somewhere between fifty and sixty thousand deaths. The entire country would follow the north into lockdown on March the 9th.
Italy had leapfrogged China to put nearly sixty million people in lockdown, the largest lockdown in human history. It is only after the lockdowns were in effect that the excess mortality appeared.
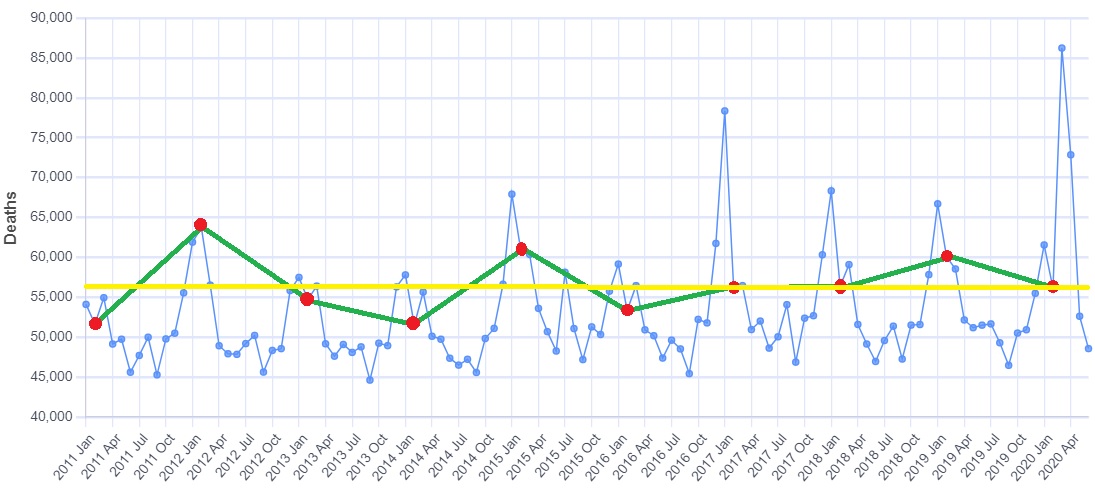
The red dots in the graph are each February, the yellow line is set at the level of February 2022. No excess mortality is detectable.
As explored in Chapter One, excess deaths in Italy were severely imbalanced towards the north of the country and likely substantially iatrogenic in nature.22
Central to Italy’s lockdown policy was Health Minister Roberto Speranza. Speranza was labelled ‘the most left-wing health minister in Italian history’.23 In October 2020, he published a book, Because we will Heal: From the Hardest Days to a New Idea of Health. The book was written during the summer, when excess mortality in Italy had receded. It was hastily withdrawn from sale due to the death rate spiking again that same month. Ostensibly this was because Speranza was too busy to devote time to presentations, but it has never gone back on sale, indicating the premature celebration of success had become embarrassing.24
Attorney Michael Senger, author of Snake Oil: How Xi Jinping Shut Down the World, proposes that Speranza might have scrapped his book due to it being too candid about his ideological reasons for locking sixty million people down.25 Speaking of the Lombardy and Veneto lockdown, Speranza writes:
‘This is a measure with worrying implications for the economic and social fabric, but also with a terrible symbolic impact. Restricting citizens’ freedom of movement, sending the army to check that closures are respected. Could the protection of the right to health, recognized by Article 32 of the Constitution, lead us to restrict other fundamental rights guaranteed by the Constitution? And then, will this type of intervention really work, to stop the contagion? No other Western country has yet experienced this virus and the management strategies it requires. The only precedent we can look to is China, with a very different cultural, political and institutional model from ours. In Italy, everyone has been saying for weeks, it would be impossible to do what China has done. But what if it were necessary?’26
In spite of Speranza describing himself as ‘a staunch rationalist’ who has a ‘true faith in science’,27 it is clear that no science underpinned Italy’s lockdown, only the recommendation of the Chinese Communist Party. One study was commissioned, using Chinese data, but was never published.28
Speranza’s book reveals his ideological drives:
‘I am convinced that we have a unique opportunity to entrench a new idea of the left, based on a commitment that today everyone recognizes is needed: to defend and relaunch fundamental public goods’
‘We have experienced unbridled individualism, we have undergone its economic and social translation: neoliberalism as well so unbridled.‘
‘Individualism has weakened social networks and fragmented representation. It was thought that the state was no longer needed, that it should be reduced to a minimum.That all his interference was a nuisance because society and the economy were able to regulate themselves. They just had to be left “free.”’
‘The months of Covid, however, have accelerated a rethinking process of which some first signs were already visible. We have rediscovered how important fundamental public goods are, starting with the protection of health. For the first time, after many years, the left is not going against the wind. We have been in the long phase in which history seemed to go in the direction of neoliberal individualism, and in our going against the wind, looking for the route, fighting against solutions that were a bit messy and that had little to do with values of the left, in Italy we have experienced a painful split in the main center-left party. Today things are changing and an idea of the left can be reaffirmed starting from fundamental public goods and a new role of the state.’29
As China made unthinkable lockdowns possible in Italy, so Italy opened the possibility for the rest of the world.
Suddenly the World Health Organization changed its tune. Abandoning it’s pandemic preparedness advice of only five months earlier declared:
‘The measures China has taken are good not only for that country but also for the rest of the world.’30
This was at a time when China was reporting one hundred and seventy deaths from COVID-19 (not enough to make a dent in typical pneumonia deaths from Hubei province) and welding people inside their homes, causing some to be burnt alive.31
WHO director-general Dr. Tedros Adhanom Ghebreyesus, a man who had once been a member of the most oppressive governments in the world,32 now said:
‘In many ways, China is actually setting a new standard for outbreak response. Our greatest concern is the potential for the virus to spread to countries with weaker health systems, and which are ill-prepared to deal with it.’33
On the 24th of February, the World Health Organization declared:
‘China didn’t approach this new virus with an old strategy for one disease or another disease. It developed its own approach to a new disease and extraordinarily has turned around this disease with strategies most of the world didn’t think would work . . . What China has demonstrated is, you have to do this. If you do it, you can save lives and prevent thousands of cases of what is a very difficult disease.’34
Scientists who had been pro-lockdown for years now seized the opportunity.35 Neil Ferguson led a study on case rates in the lockdowned town of Vo’, Italy.36 Professor Ferguson claimed to show that it had been effective, which influenced the decision to lockdown all of Italy on March the 9th. The study was based on testing for infections, which were demonstrably in decline before the lockdown had started.37 To quote Michael Senger:
‘Ferguson justified the lockdown of the United Kingdom based on the lockdown of Italy, which had in turn been justified with a false study led in part by Ferguson himself.’38
Much like Roberto Speranza with China, Professor Ferguson credited Italy with making lockdowns possible:
‘It’s a communist one party state, we said. We couldn’t get away with it in Europe, we thought… and then Italy did it. And we realised we could.’39
White House Coronavirus Response Coordinator Dr. Deborah Birx wrote of how she became convinced of the need to lockdown after seeing videos from China—videos that were soon conclusively proven to be propaganda:40
‘We had to make these palatable to the administration by avoiding the obvious appearance of a full Italian lockdown. At the same time, we needed the measures to be effective at slowing the spread, which meant matching as closely as possible what Italy had done—a tall order.’41
The initial justification for lockdowns was not to stop the virus passing through society, but to slow the spread so that hospitals would not be overwhelmed. Birx also admits that the ‘fifteen days to stop the spread’ was a lie:
‘No sooner had we convinced the Trump administration to implement our version of a two-week shutdown than I was trying to figure out how to extend it. Fifteen Days to Slow the Spread was a start, but I knew it would be just that. I didn’t have the numbers in front of me yet to make the case for extending it longer, but I had two weeks to get them. However hard it had been to get the fifteen-day shutdown approved, getting another one would be more difficult by many orders of magnitude.’42
By April, more than half the world’s population—some 3.9 billion people—had been placed into lockdown.
It is clear that this policy, created and promoted by one of the world’s most authoritarian regimes, had no real scientific underpinning and was pushed for ideological reasons by people who were entirely aware of the devastating consequences.43 Even if there hadn't been a deadly virus circling the world, lockdown policies—taken in totality—were guaranteed to kill millions of people. Some of those deaths would be realised immediately, such as the ones arising from denial of healthcare, others would take weeks, such as starvation in the Third World, whilst still more would manifest over years to come, such as cancer deaths and the loss of services due to economic contraction. To say it again: all of this was entirely apparent at the time.44
To quote Michael Senger once more:
‘The world has been fighting a virus from China with a public health policy from China that transforms the world into China.’45
How could this be justified? Only through the claim that lockdowns would save more lives than they cost. Absent evidence, this is simply a gamble, so was it a gamble that paid off?
Lockdown efficacy
There are no shortage of claims that lockdowns saved millions of lives.46 If a strong form of the iatrogenic hypothesis explored in Chapter One is correct, whereby deaths attributed to COVID-19 were overwhelmingly caused by changes to medical systems, then lockdowns obviously did not save a single life. Their power could only have been destructive.
A case for this can certainly be made from the data. Various scientific studies have found evidence that the COVID-19 virus was present around the world for months before its sudden emergence as a killer. In Italy, it has been identified as far back as September 2019.47 This seems hard to reconcile with the fact that none of the countries supposedly strongly affected by COVID, saw any increased mortality prior to March 2020. More specifically, they did not see any prior to the implementation of lockdowns.
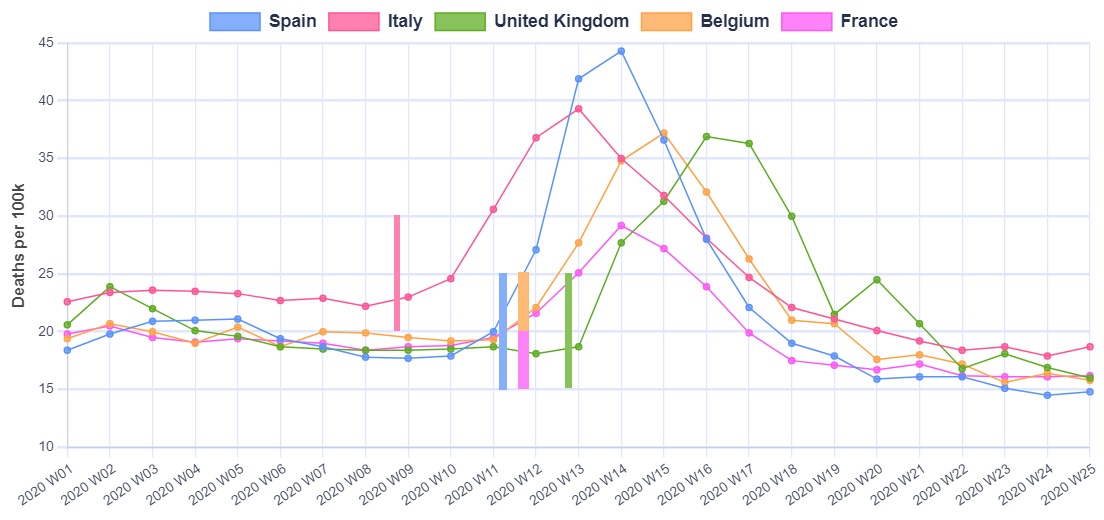
The graph below shows five European countries that experienced high excess mortality beginning in March 2020. The vertical bars indicate the various dates these countries imposed stay-at-home orders. This is an imperfect starting point, as it is not the act of staying home that causes excess deaths, but as the most extreme measure, stay-at-home orders are likely to have come shortly after changes to medical systems.
It is clear that lockdowns always precede excess mortality. Italy went into lockdown earlier than the other countries, and its excess deaths came proportionately earlier too. At the other end of the scale, the United Kingdom instituted lockdowns last, and was the last to see a mortality spike.48
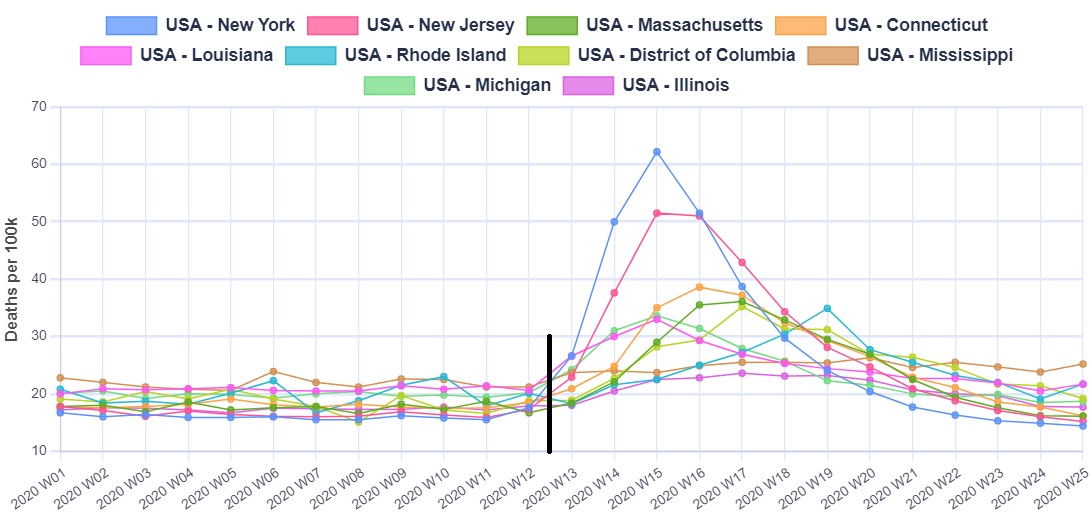
The picture is similar in the United States. The graph below shows the ten States which initially had the highest excess mortality. The black line is the date States issued stay at home orders or recommendations (plus or minus a couple of days). The same pattern as seen in Europe emerges, where no excess deaths are visible prior to lockdown, but a sudden spike comes immediately after. Europe's death spikes come just a few days prior, with the UK being slightly later.49
By June of 2020, Dr. Anthony Fauci had been thoroughly won over to the lockdown cause, saying:
‘If you look at the data, now that papers have come out literally two days ago, the fact that we shut down when we did and the rest of the world did, has saved hundreds of millions of infections and millions of lives.’50
Dr. Fauci is most likely referring to a collection of papers published just a few months after lockdowns were mandated, that claimed to demonstrate this saving of ‘millions of lives’. The papers were based on modelling speculative predictions of how COVID might travel and how lethal it might be. They did not take into account iatrogenic deaths or the more long term deaths that would be caused by lockdowns. They also do not seem to comport well to observations of the real world.51
If lockdowns really had saved millions of lives in such a short period, then the effect would be impossible to miss. Indeed the world’s media predicted as much at the time.52 Any country eschewing this policy would suffer cataclysmic consequences, unmissable in both the data and anecdotal observations.
Is such a cataclysm visible?
The ‘Deaths Soar In Country That Didn’t Lock Down’ quotation that opens this chapter is a CNN headline referring to Sweden. It is true that Sweden did not lockdown and deaths did indeed soar, but does the relationship that CNN implies actually exist?
If Sweden is added to the previous graph of the five European countries that did lockdown, it is clear that the initial period of excess mortality rose and fell away again at about the same rate.53 This means that, in spite of understandable public perception to the contrary, lockdowns cannot be credited with bringing the death rate under control.
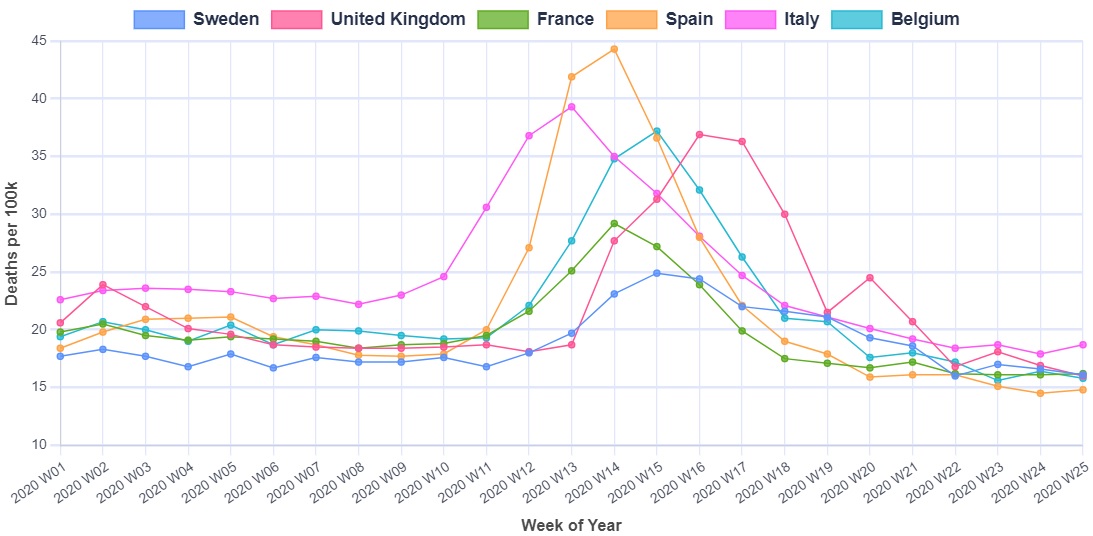
Over half of the Swedish deaths at this time occurred in nursing homes, and it is clear iatrogenic factors played a substantial role.54 The country experienced no excess mortality in the under seventy fives during 2020, so whilst there are doubtlessly many things Sweden could have done (or better to say, not done) to reduce their excess mortality, it is unclear how locking down younger people could have contributed.55
Supporters of lockdowns have claimed that Sweden should be compared to its Nordic neighbours, rather than Europe in general. When this comparison is made, it is clear Sweden did comparatively badly during 2020, with two big spikes in excess mortality.56
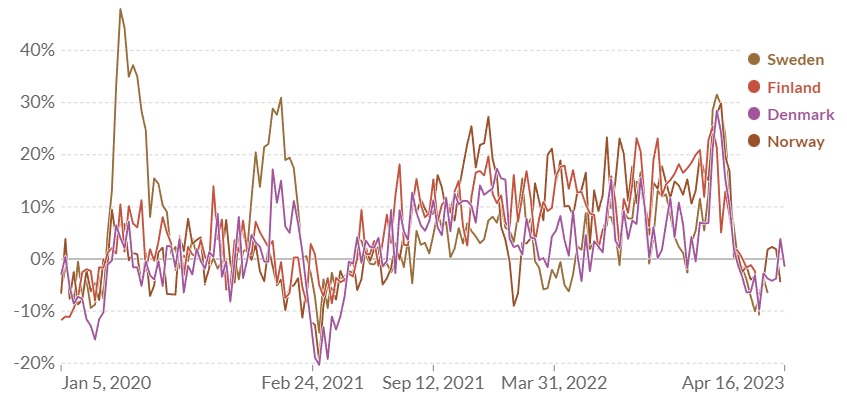
From February of 2021 onwards however Sweden’s excess was consistently lower than its neighbours. By June of 2022, the UK Office of National Statistics reported that Sweden was tied with Norway for lowest excess deaths in Europe since the beginning of the pandemic period.57
Of course many countries instituted stay-at-home orders and did not instantly see an increase in excess mortality. It is claimed this is because they locked down before the virus had time to spread, and other countries would have had the same results if only they’d locked down sooner. To justify this claim however, it would have to be known what medical policies these countries had in place. An absence of excess mortality would indicate that, at least at this stage, they were not denying medical care to their elderly the way the, for example, United Kingdom was.58
The United States provides an interesting—yet challenging—basis for comparison. Different States locked down in different ways for different periods of time. The bar chart below contains the deaths attributed to COVID-19 as of August 19th 2020, essentially the point where most States had concluded their first phase of lockdowns.59 The red dots are the states considered to have not locked down, or at least where restrictions were mildest:60
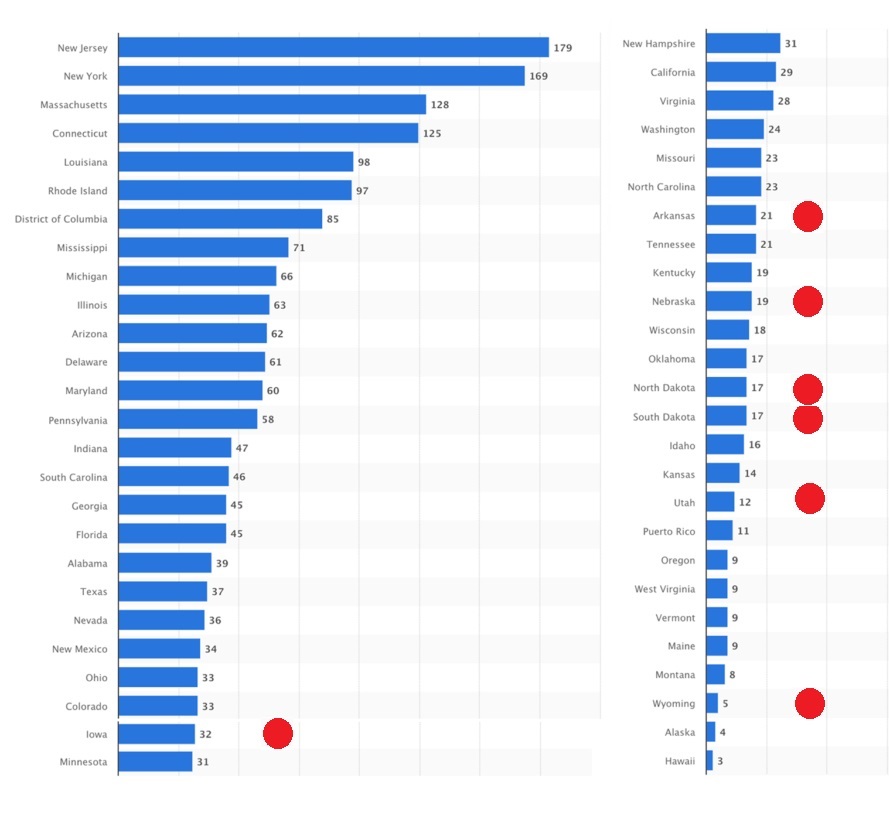
It can of course be argued that not enough time had elapsed to gain a clear picture, this graph is clearly not what the lockdown supporters were claiming would happen in March 2020.
After two years had elapsed, a working paper published in the National Bureau Of Economic Research found that excess mortality was: ‘greater in US states where obesity, diabetes, and old age were more prevalent before the pandemic’, and that; Economic activity was less in states that had been intensive in, especially, accommodations and food. When these factors were controlled for, they found no relationship between reduced economic activity (a proxy for lockdowns) and excess mortality:61
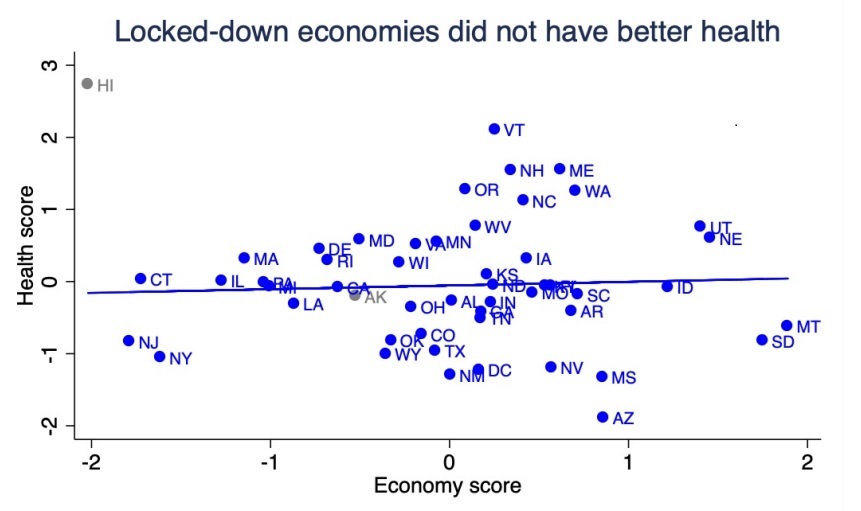
Whilst there are obviously a million ways to cherry-pick data, once pre-existing health conditions are taken into account, there seems to be no evidence that lockdown States had better health outcomes: never mind the dramatic picture we should be seeing if lockdown proponents were correct.
As one further example, Japan, although imposing border controls, did not mandate an internal lockdown. The country experienced no excess mortality in 2020, in spite of case numbers increasing. Excess deaths emerged in 2022—after a high proportion of the population was vaccinated. Prior to this, Japanese people simply didn’t die of COVID in high enough numbers to impact excess mortality.62 This is hard for not only lockdown advocates to explain—but for proponents of the viral theory in general.63, 64
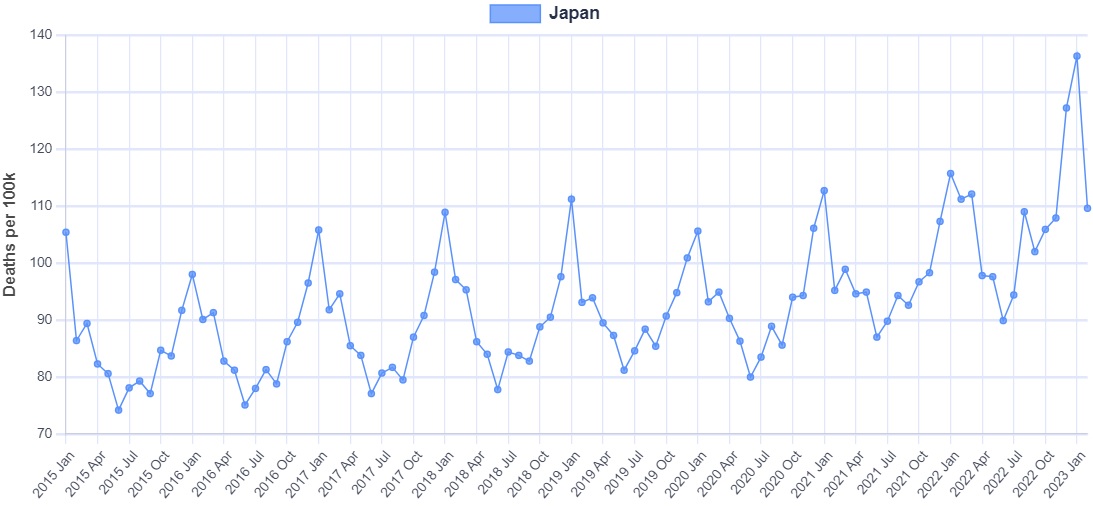
Japan did have a high level of compliance with the Government requests to minimise social contact. This might be expected, if people believe a deadly virus is being breathed out by their fellow humans, then they are likely to avoid them.
Conclusion
In an article explaining the difficulties of assessing lockdown efficacy, Associate Professor of Medicine Vinay Prasad wrote that:
‘I suspect that for many restrictions -- perhaps even most restrictions -- we will never know. We will never know, for instance, if removing the rim from a basketball hoop or closing a toboggan hill slowed SARS-CoV-2 where these strategies were deployed. For larger interventions -- mandatory business closure and stay at home orders, colloquially called "lockdowns" -- we may someday have a scientific consensus as to whether and to what degree this practice changes viral spread, but I believe that day is years away.’65
Dr. Prasad writes a perceptive and thought provoking article describing the difficulties of this kind of analysis. If he is correct that lockdowns effects, even on viral spread, are too small to be measured, then this is not a neutral conclusion, rather, it is utterly damning.
If lockdowns came at no cost, then it wouldn’t really matter if the benefit was too small to measure. We know however, that the cost was staggering. Anything less than at least equally staggering benefits then, is an unparalleled disaster. It is clear that lockdowns simply have not demonstrated anything like the kind of benefit that would justify their cost, it is not actually clear they have demonstrated any benefit at all.
Unlike the lockdown predictions, predictions of disaster clearly turned out to be true, with the UN and Oxfam reporting the impact on global poverty and food prices.66 Cancer diagnoses were missed,67 elderly people died alone.68 There are other costs too: unfortunately we do not live in a Disney movie where true love always finds a way. Missed opportunities cannot necessarily be replaced. The obstruction of lockdowns means families that would have otherwise formed, now will not. This is quite an incredible thing to take away from people.69
We also do not live in a world where resources can be brought forth by magic. Resources consumed today are simply not there for tomorrow. Lockdowns are a double-whammy, where resources are consumed to pay for people to not create more resources. Countries spent simply vast amounts of money furloughing workers who—as Sweden shows—were at no risk from COVID relative to other health risks they may face. Even if it were possible to keep a country ‘COVID free’ with such a policy, it will simply be paid for in the future when those resources, already spent, are not there to invest in healthcare targeting cancer and heart disease etc. This not to mention any other area of life. There is no world in which it makes sense to redirect resources away from more serious and toward less serious threats to health. This is exactly what governments around the world have done. The United Kingdom now has a consistently higher excess mortality rate than pre-COVID, and this is attributed to strain on the NHS. People are now dying as the resources that would have treated them have already been consumed protecting them from something that posed no comparative threat.70
This chapter can only conclude with Tacitus’ famous observation of the Roman Empire, that ‘where they make a desert, they call it peace.’71
Questions for the State
What was the scientific basis for the state’s decision to implement a lockdown?
What science emerged to support the continued use of lockdowns?
Given the evidence presented in this document, does the state still consider lockdowns to be a efficacious strategy, where the benefits outweigh the harms?
Given that, as in other places, deaths attributed to COVID-19 came after a lockdown was instituted, can the state confirm that these deaths did not come about as a result of changes to the health service, as was seen in the UK and other countries?
Given the evidence presented in this document, would the state consider employing lockdowns in the future?
How did the state perform a cost benefit analysis of lockdowns? How does the state assess the costs versus the benefits now?
How many lives does the state estimate were saved by the lockdowns it implemented?
How many lives does the state estimate were or will be lost because of the lockdowns it implemented?
Four. Vaccination
‘When we finally do, God willing, get access to a vaccine, who’s going to take the shot? Who’s going to take the shot? Are you going to be the first one to say “sign me up, they now say it’s okay”?’
Nominee for President, Joe Biden1
‘My message to unvaccinated Americans is this: What more is there to wait for? What more do you need to see? We’ve made vaccinations free, safe, and convenient. The vaccine has FDA approval. Over 200 million Americans have gotten at least one shot. We’ve been patient, but our patience is wearing thin. And your refusal has cost all of us. So, please, do the right thing. But just don’t take it from me; listen to the voices of unvaccinated Americans who are lying in hospital beds, taking their final breaths, saying, “If only I had gotten vaccinated.” “If only.”’
President Joe Biden2
It’s a high bar, but the vaccination program was possibly the most contentious aspect of the whole COVID-19 era. Lockdowns inevitably end, masks can be taken off, but being compelled to have something injected into one’s body—for many people this was an affront too far.
For others, the refusal of a seeming minority to embrace science and undergo a demonstrably safe, effective and minor medical procedure, spoke to a selfish ignorance in that portion of the population.
A tension was established, from which a certain divisive nastiness was birthed. It is disappointing, but perhaps not surprising to see a politician like Joe Biden use his position to exacerbate this divisiveness. More surprising was previously anti-establishment radical voices like Noam Chomsky, calling for the unvaccinated to be ‘isolated from society’, and stating how they acquired food was ‘their problem.’3
This divisiveness spread into society, with over a quarter of American voters favouring detention centres for the unvaccinated and criminal penalties for merely questioning the efficacy of the shots.4
In Britain, Tony Blair advocated the creation of a two-tier society, with the vaccinated enjoying more freedoms (or less restrictions). His institute advocated for ‘a globally interoperable system of health passes’.5
Nurses, the heroes of 2020, had become villains by 2021, with thousands of them facing the sack for refusing the jab.6
For now, this two tier society has collapsed, its remnants swept away in lawsuits and embarrassing climb downs.7 It leaves a more bitter and divided society in its wake, and will doubtlessly return at some future point.
So how did we get to such a dystopia?
It is perhaps helpful to recognise that this situation is not new. For well over a century, states around the world have shown great favour to vaccinations as a preferred public health measure. Whatever good or ill Edward Jenner’s creation brought into this world, efforts to mandate vaccines have always engendered division; with fines, seizures of property and imprisonment being employed to coerce the reluctant. A illustrative, yet seemingly not unique, example was printed in The New York Times in 1901:
‘There was a lively time in the works of the American Tobacco Company this afternoon, when the 350 girls employed objected to being vaccinated by the physicians sent there by the health officers . . . When the health officers went to the factory the girls were informed that every one of them would have to be vaccinated. Some of them fainted, others became hysterical, and there was a general rebellion. About 200 of them, led by Florence Haskell, attempted to get out of the works, but they found all the exits locked. The police were called and the work of vaccination began. Some of the girls fought the officers and were led up to the physicians screaming, struggling, and kicking. The greatest excitement prevailed and all work had to be suspended. At one time some of the girls threatened to destroy the factory if they were not allowed to go out, but all were finally vaccinated.’8
Even the evidence cited by proponents and opponents of vaccination differs. To take measles as an example, proponents might point to the utter collapse in the case rate after the introduction of vaccination as proof positive of its efficacy:9
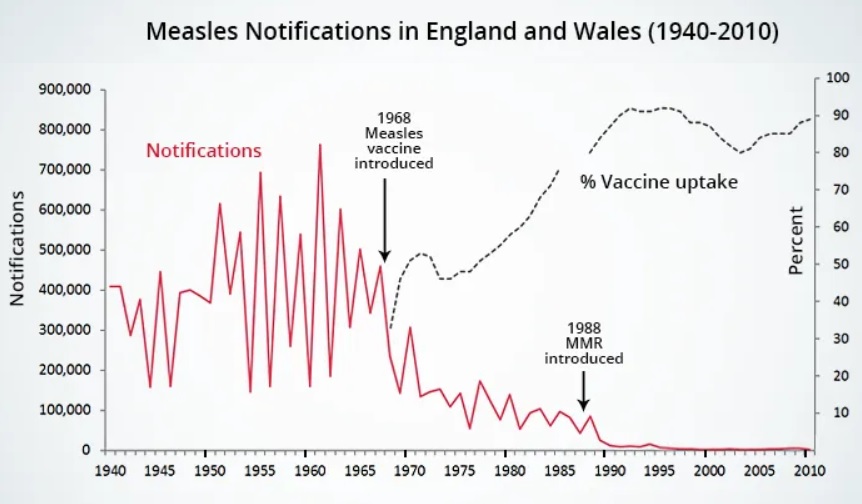
Where as opponents are likely to point to the death rate from the disease, pointing out it had collapsed prior the the vaccines introduction:10
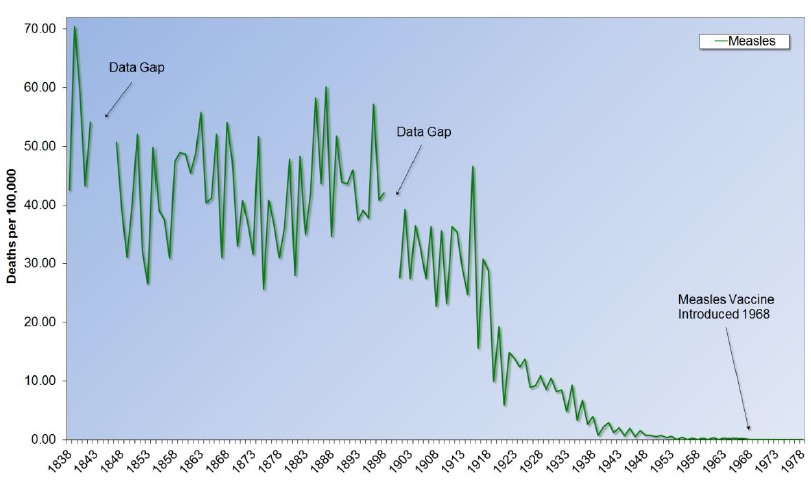
The same pattern of pre-vaccine decline is present for many infectious diseases, including scarlet fever, for which there is no vaccine:
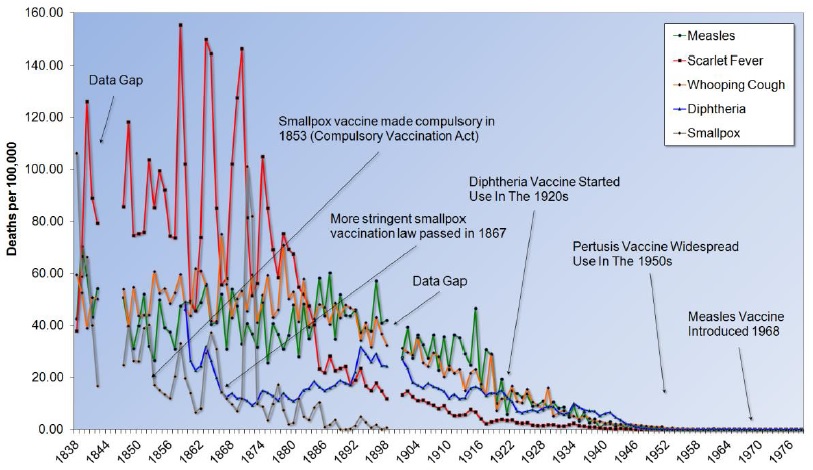
The decline in measles deaths is also concomitant with the decline in deaths from scurvy, which suggests what we are really seeing is a general decline in nutritional deficiencies through the 20th century.

It is with this history we arrive at the COVID-19 vaccine debate.
At some point in 2020, the purpose of lockdowns shifted from slowing the spread, to keeping everyone safe until a vaccine was available. In criticising the Great Barrington Declaration’s call for focused protection,11 WHO director-general Dr. Tedros Adhanom Ghebreyesus claimed that herd immunity is reached through vaccination, not by exposing people to a virus. In October 2020 he said:
‘Allowing a dangerous virus that we don't fully understand to run free is simply unethical. It's not an option,’12
Dr. Anthony Fauci had now shifted from a lockdown sceptic, to believing they were necessary until a vaccine was available:
‘You use lockdowns to get people vaccinated so that when you open up, you won't have a surge of infections, because you're dealing with an immunologically naive population to the virus, because they've not really been exposed because of the lockdown.’13
Whilst Bill Gates, whose Foundation substantially contributes to the World Health Organization, said:
‘One of the questions I get asked the most these days is when the world will be able to go back to the way things were in December before the coronavirus pandemic. My answer is always the same: when we have an almost perfect drug to treat COVID-19, or when almost every person on the planet has been vaccinated against coronavirus.’14
In spite of predictions that it would take at least eighteen months to produce a vaccine,15 the first vaccine for COVID-19 was actually available in China as early as June of 2020, with the Russian’s developing one by August. In the West, Pfizer, AstraZeneca and Moderna had vaccines by December, with Johnson & Johnson following on in February 2021.16
The arrival of vaccines was, of course, treated with jubilation, and the increasingly coercive rollout began. Yet in spite of the ‘we’re all in this together’ rhetoric, there was no particular reason to be trusting of pharmaceutical companies—or their regulators—based on track record.17 Perhaps the most famous and egregious case in recent years is that of Merck’s arthritis drug, Vioxx. Merck’s failure to report problems during the trial led to the drug causing an estimated 160 thousand heart attacks and strokes in the general population.18 The US Food and Drug Administration (FDA) was found to be complicit in the dangerous drug’s approval.19 The FDA has often been criticised for operating a ‘revolving door’ with the pharmaceutical industry.20
In 2004, Johnson & Johnson agreed to pay up to 90 million dollars to settle lawsuits around their heartburn drug, Propulsid. Johnson & Johnson illegally promoted the drug for children and suppressed studies demonstrating its dangers. Claims indicated that up to three hundred people died and as many as sixteen thousand were injured. The New York Times described this as:
‘A pharmaceutical company trying to save a lucrative drug in the face of growing evidence of harmful side effects.’21
In 2009, Pfizer was forced to pay ‘the biggest criminal fine in US history as part of a $2.3bn settlement with federal prosecutors for mis-promoting medicines and for paying kickbacks to compliant doctors.’22 One Pfizer sales rep turn whistleblower said of the lawsuit:
‘In the Army I was expected to protect people at all costs, at Pfizer I was expected to increase profits at all costs, even when sales meant endangering lives.’23
Pfizer is also implicated in bribing officials in order to carry out drug trials on children in the Third World.24
In 2010, AstraZeneca was fined 520 million dollars for prompting an antipsychotic medication for off label and seemingly unrelated conditions.25 AstraZeneca was again sued in 2018 for similar practices in the State of Texas, this time for 110 million dollars.26 In 2021 the company was once again sued by a sales rep, who claimed the company fired her for refusing to promote drugs in a misleading manner.27
With this background, and billions of dollars on the line, there is every reason to have a starting point of cynicism regarding claims of both safety and efficacy.
The trials
Trials for the various vaccines claimed to show significant reductions in symptomatic cases of and hospitalisations from COVID-19.28 The presentation of the trials could be misleading, for example, when AstraZeneca claimed their vaccine was 100% effective against severe disease and hospitalisation, people probably did not imagine this meant that in a study containing over 20 thousand people, a total of 5 in the control group were hospitalised whilst none in the vaccine group were.29
Pfizer used a similar technique of presenting relative risk reduction to claim their vaccine was 95% effective, when the absolute risk reduction was less than 1%.30 Whilst arguments for either way of presenting data can be made, more concerning was the exclusion of 311 (1.4%) vaccine recipients as compared to only 61 (0.3%) placebo recipients from the trial for ‘protocol deviations’, an imbalance that cannot realistically happen by chance and suggests the study was not truly blind.31
Confirmation of this came when a whistleblower provided the British Medical Journal with ‘dozens of internal company documents, photos, audio recordings, and emails’, demonstrating falsified data, unblinded patients and slowness in following up on adverse events reported in Pfizer’s trial. Additionally, not all participants exhibiting symptoms of COVID-19 were tested. The FDA was informed of these issues in advance of authorisation, but took no action.32
An independent reanalysis of both the Pfizer and Moderna trials found a statistically significant serious adverse events rate in the vaccine groups.33
Safe and Effective?
What happened when vaccines were rolled out? Given the criminal records of the companies developing them, apparent problems with the trials and record breaking development time, a prudent person might have kept their expectations low. Such caution would have been unnecessary however, as the vaccines appeared to be nothing short of a medical miracle.
The US Centers for Disease Control reported that unvaccinated people were 14, 20, or even 97 times more likely to die of COVID-19, depending on how you cut the numbers.34 The Office of National Statistics (ONS) echoed this trend in the UK.35 By December 2021, a study in the Lancet claimed the vaccines had saved nearly 20 million lives that year.36, 37
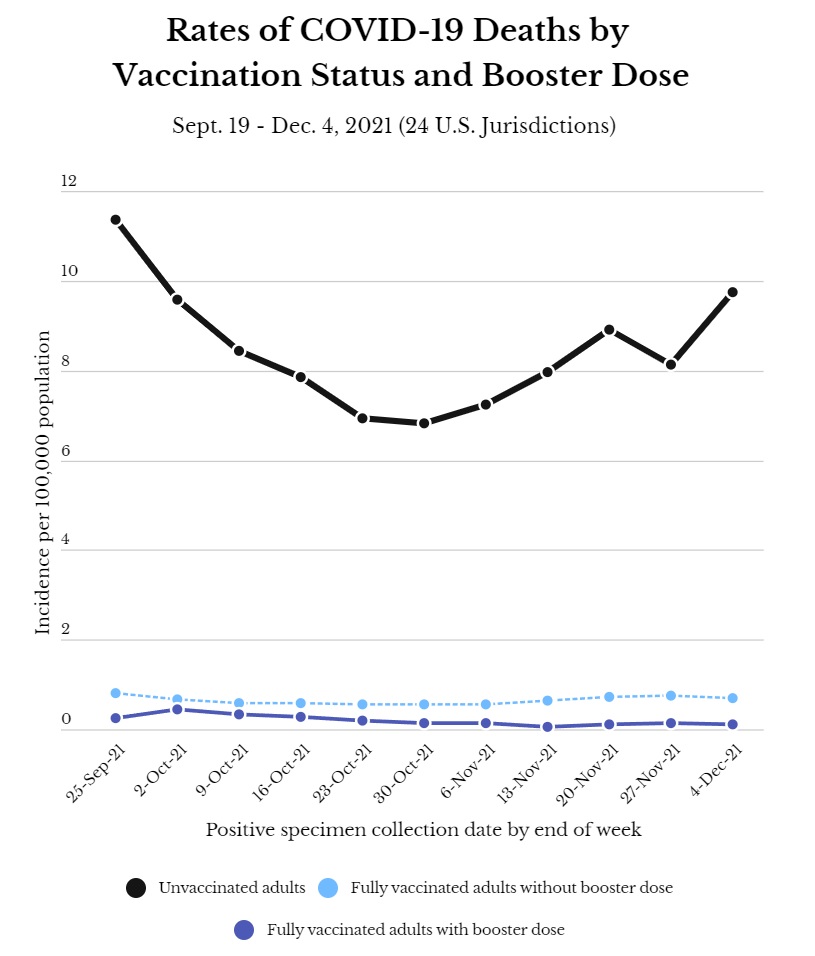
If this data is accurate then not only are the vaccines truly life saving, but the iatrogenic hypothesis explored in Chapter One must be severely limited as an explanation for excess mortality. Whilst there certainly must have been iatrogenic deaths during the COVID era, the virus must have caused the lion’s share of the excess mortality. This brings up a contradiction, as we explored how the geographic and temporal movement of the mortality spikes is inconsistent with what would be expected from a virus.
On the other hand, if the iatrogenic hypothesis is correct, then the vaccines simply cannot have been saving all these lives. We also see an unprecedented safety signal appearing on the US Vaccine Adverse Event Reporting System (VAERS) and the British Yellow Card system.38
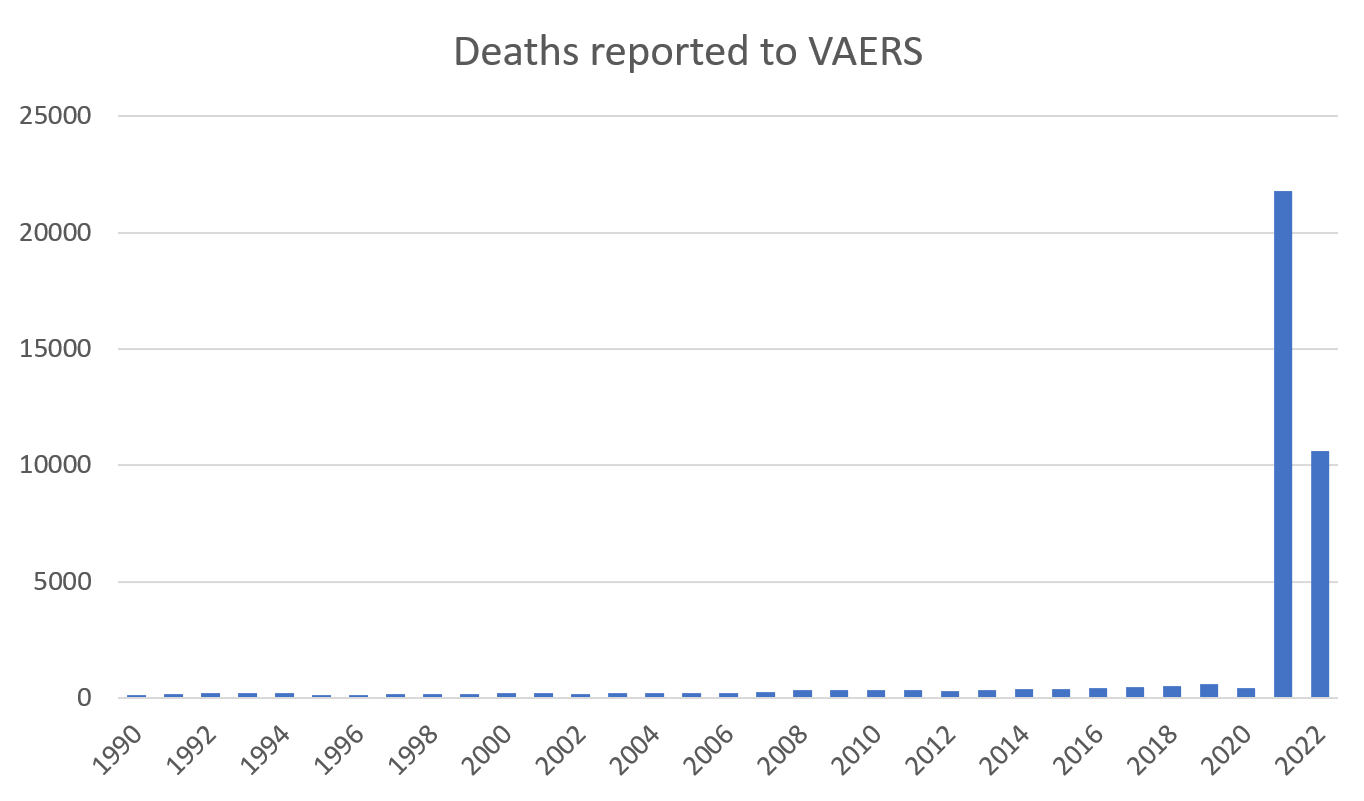
As it’s very unlikely both these pictures could be accurate, something has to give. It could be that the vaccines are being observed much more closely, due to their emergency use authorisation, and that’s why there are so many more adverse events being reported.39 The other possibility is that the vaccines aren’t so much a miracle, as a magic trick.
It turns out there are several statistical sleight of hands that can be employed to create illusions regarding vaccine safety and efficacy. Norman Fenton was Professor Emeritus of Risk at Queen Mary University of London. He and his team have demonstrated how these techniques have been employed to just such an end. The following sections shall draw heavily on their work.40
Undercounting the unvaccinated
A statistical distortion will arise if the estimation of the proportion of the population that is unvaccinated is incorrect. If the estimation is too low, the vaccine will appear more effective than it really is. The opposite is true for an excessively high estimation, which would make the vaccine appear less effective.
To understand the implications of this, it is perhaps helpful to start with an abstract example, then move to examine the situation in the real world.41
Imagine a country of 10 thousand people, where 1% of them (100 people), die from a virus. Medical records reveal that of these 100 people, 80 were vaccinated and 20 weren’t. This information alone doesn’t tell us anything about the efficacy of course, we can only assess that if we know how many people in the total population were vaccinated to begin with.
If the country’s Statistics Office announces that only 10% of the population were unvaccinated; that means 1,000 people were not, compared to 9,000 who were. This would mean a disproportionately high number of the unvaccinated had died, a mortality rate of 200 per 10,000, as compared to just 89. Assuming all other factors are equal, this is a clear victory for the vaccine.
Now imaging the Statistics Office confess to a miscalculation. In their revised figures, it turns out 30% of the society was unvaccinated! The situation now flips, with the mortality rate being 67 for the unvaccinated, and 114 for the vaxxed. It turns out that the vaccine was not only useless, it was actively harmful.
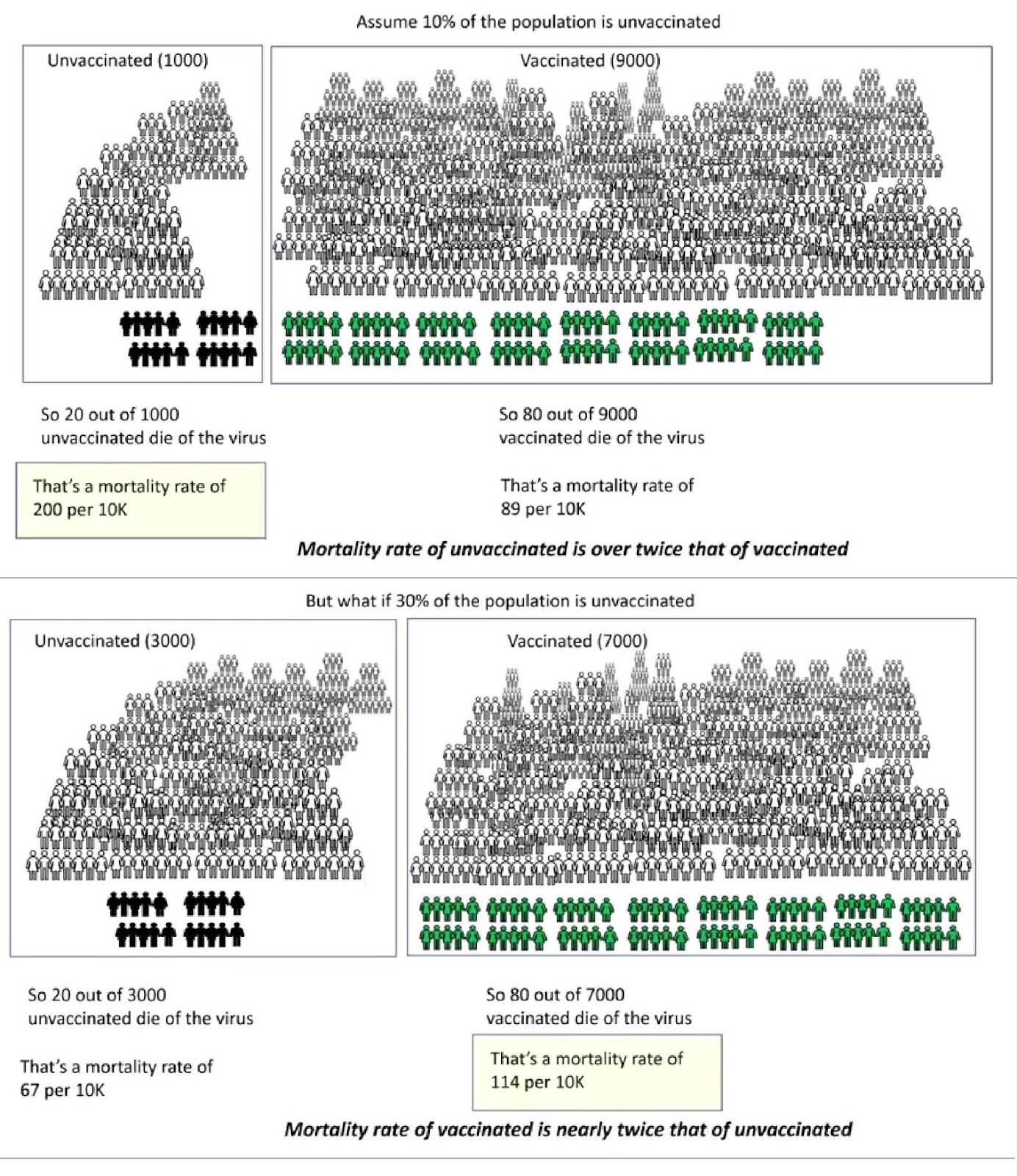
In a formal letter of complaint to the United Kingdom’s Statistics Regulator, Professor Fenton and his colleagues alleged that this is exactly what the Office of National Statistics has done.42 They highlight a disparity, where the ONS claims 8% of English people are unvaccinated, but the UK Health Security Agency estimates approximately 20%. The Regulator acknowledged this point, recognising that ONS data excluded 21% of the population who were not on the 2011 census and registered with a GP. These people are likely to be both younger in age and unvaccinated.43
The BBC used the ONS ‘8%’ figure for their documentary Unvaccinated. This was in spite of conducting their own survey which found 26% of adults were unvaccinated.44
The Statistics Regulator pointed out that the ONS makes clear that their analysis ‘is not intended to be, nor is it appropriate for, understanding vaccine effectiveness.’45 The Regulator agrees with this assessment, however Professor Fenton demonstrates that ONS data has been used exactly for this purpose by both the media and the British Government.46
When is a vaccinated person unvaccinated?
A further issue identified by Professor Fenton’s team is that of the vaccines being a little too ‘safe and effective’. Whilst this may sound like no bad thing, when the point of impossibility is reached, it rather suggests there is something wrong with the numbers.
The table below, taken from ONS data, compares the age adjusted mortality rate between the vaccinated and unvaccinated in England. Many people would not be surprised to find the unvaccinated suffer thirteen times more COVID associated deaths than the vaccinated. What should surprise everyone however, is that they also suffer 65% more non-COVID deaths.47
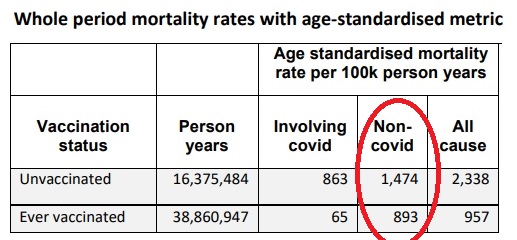
This is certainly a head scratcher. Attempts to explain this phenomenon have included the idea of long COVID, the proposition that COVID-19 is causing serious long term health problems, leading to more fatal strokes and heart attacks in the unvaccinated. The studies underpinning this however are guilty of comparing dissimilar population groups: people who were sufficiently ill with COVID to seek medical attention, with those who never knowingly caught the virus.48
If we look just at the last month of the ONS report, the gap between vaccinated and unvaccinated has all but closed in both non-COVID deaths and all cause excess mortality. Professor Fenton’s team suggests this indicates the anomalies might be disproportionately due to misclassification errors that occurred early on in the study period, which were corrected towards the end. What’s especially interesting, is that in all but one category, deaths of the unvaccinated are considerably lower that of the vaccinated.49
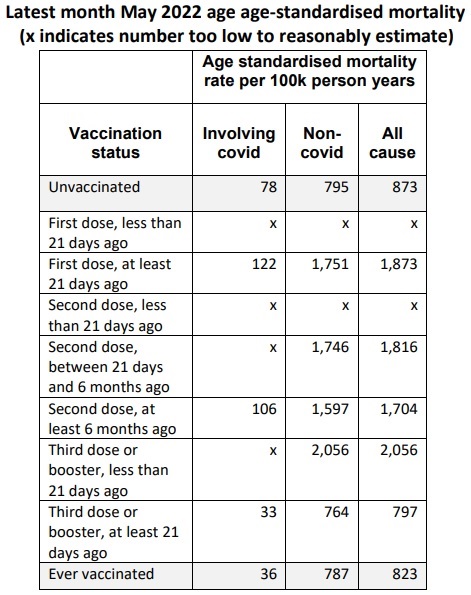
In the decade before COVID, England and Wales averaged around 973 deaths per 100 thousand people per year.50 According to ONS data, even when COVID deaths are factored in, the vaccinated are now dying at a level below that average. Whereas the unvaccinated population are dying from non-COVID illnesses at a 50% higher rate than prior to the pandemic period. It could be that the vaccinated are simply a far healthier cohort of the population than the unvaccinated to begin with, however this would mean that all observation studies and all Government data would be significantly overestimating vaccine efficacy by not accounting for this bias. Dr. Fenton’s team comment:
‘It has been suggested that the anomalies are the result of healthy vaccinee selection bias and population differences. However, we show why the most likely explanations for the observed anomalies are a combination of systemic miscategorisation of deaths between the different categories of unvaccinated and vaccinated; delayed or non-reporting of vaccinations; systemic underestimation of the proportion of unvaccinated; and/or incorrect population selection for Covid deaths. We also find no evidence that sociodemographic or behavioural differences between vaccinated and unvaccinated can explain these anomalies.’
This graph displays the effect.51
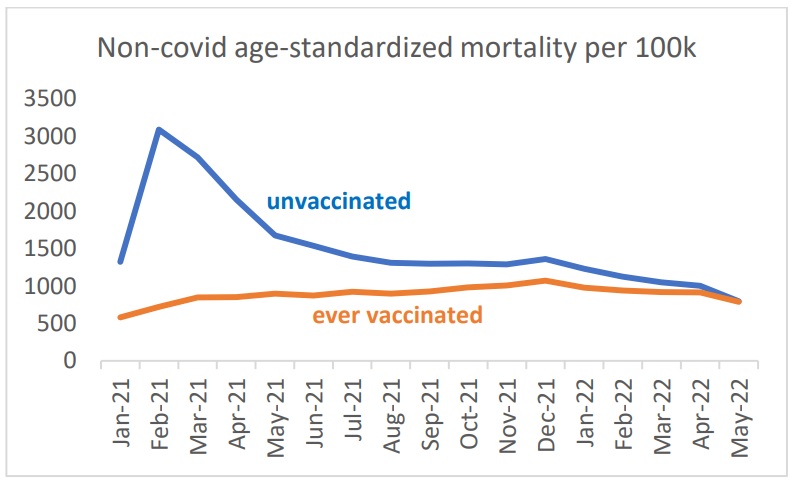
Notice the sharp rise in non-COVID deaths amongst the unvaccinated, concomitant with the vaccine’s roll out. This caused Professor Fenton to quip that:
‘When you roll out the vaccine, all the unvaccinated suddenly drop dead.’52
Professor Fenton’s team claim the explanation for this is that the vaccinated are simply being misclassified as unvaccinated for a period of three weeks after they take the shot. There is a legitimate reason for this: the COVID vaccines are thought to require two or three weeks to take effect. If a researcher is looking to assess vaccine efficacy then it would be sensible to only consider a person vaccinated after this period has elapsed. This approach however obviously obscures any safety signal the vaccine is giving off.
Whether the ONS classified vaccine status in this delayed manner is contentious. In response to Professor Fenton’s complaint, they reported to the UK Statistics Regulator that they do not. The Regulator accepted this and proposed a different explanation for the data.53 The ONS’s own website seems to contradict this however:
‘We calculated vaccine effectiveness for different doses (first, second and third dose or booster) and time since dose, to observe how the effectiveness changes over time. The vaccination statuses used were: unvaccinated (those with no vaccination or who were vaccinated with a first dose less than 21 days ago)’54 [Emphasis added]
This same method seems to be used in both Sweden,55 and by the US CDC:
‘Persons were considered fully vaccinated ≥14 days after receipt of the second dose in a 2-dose series (Pfizer-BioNTech or Moderna COVID-19 vaccines) or after 1 dose of the single-dose Janssen (Johnson & Johnson) COVID-19 vaccine¶; partially vaccinated ≥14 days after receipt of the first dose and <14 days after the second dose in a 2-dose series; and unvaccinated <14 days after receipt of the first dose of a 2-dose series or 1 dose of the single-dose vaccine or if no CAIR2 vaccination data were available.’56 [Emphasis added]
Dr. Fenton’s team points out that the spikes in apparently unvaccinated mortality do not coincide between different age groups, but rather follow the rollout of the vaccine to those groups. The 80+ age group was the first to be vaccinated, and, coinciding with this, they are the first to see unvaccinated deaths spike, followed by the 70s and 60s group. This is true for all cause mortality, but perhaps more tellingly, for non-COVID mortality too:57
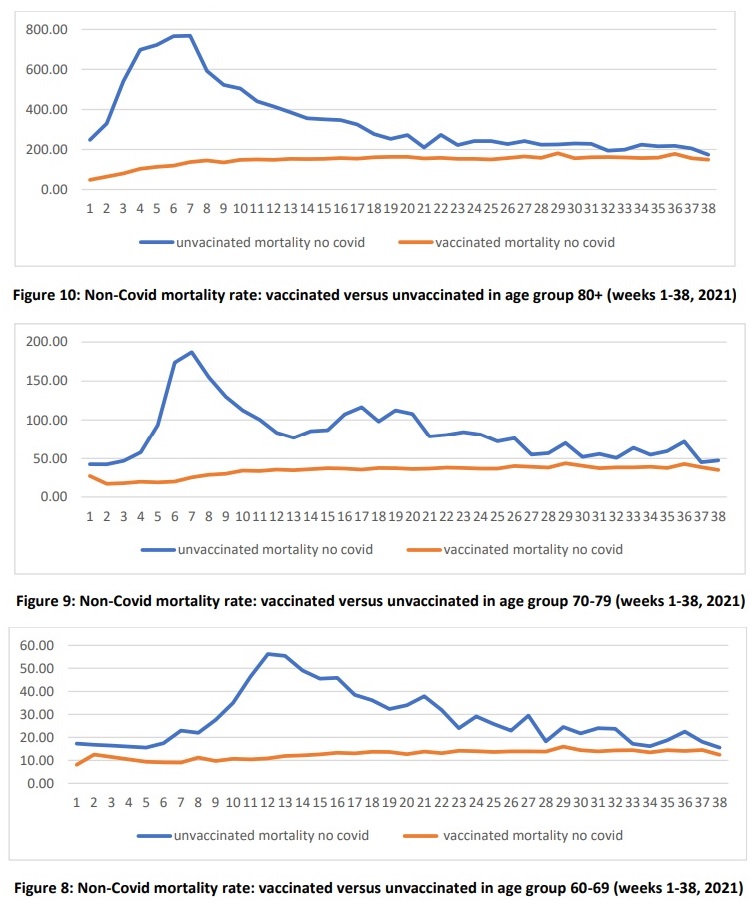
Hospital records
Through freedom of information requests, Professor Fenton’s team also identified serious problems with hospital record keeping, where patients were classified as ‘unvaccinated’ if they had not been vaccinated in that particular hospital/Trust. Alternatively, evidence was found of hospitals using the national system (NIMS), not registering any deaths in vaccinated people prior to that system coming online in June.58
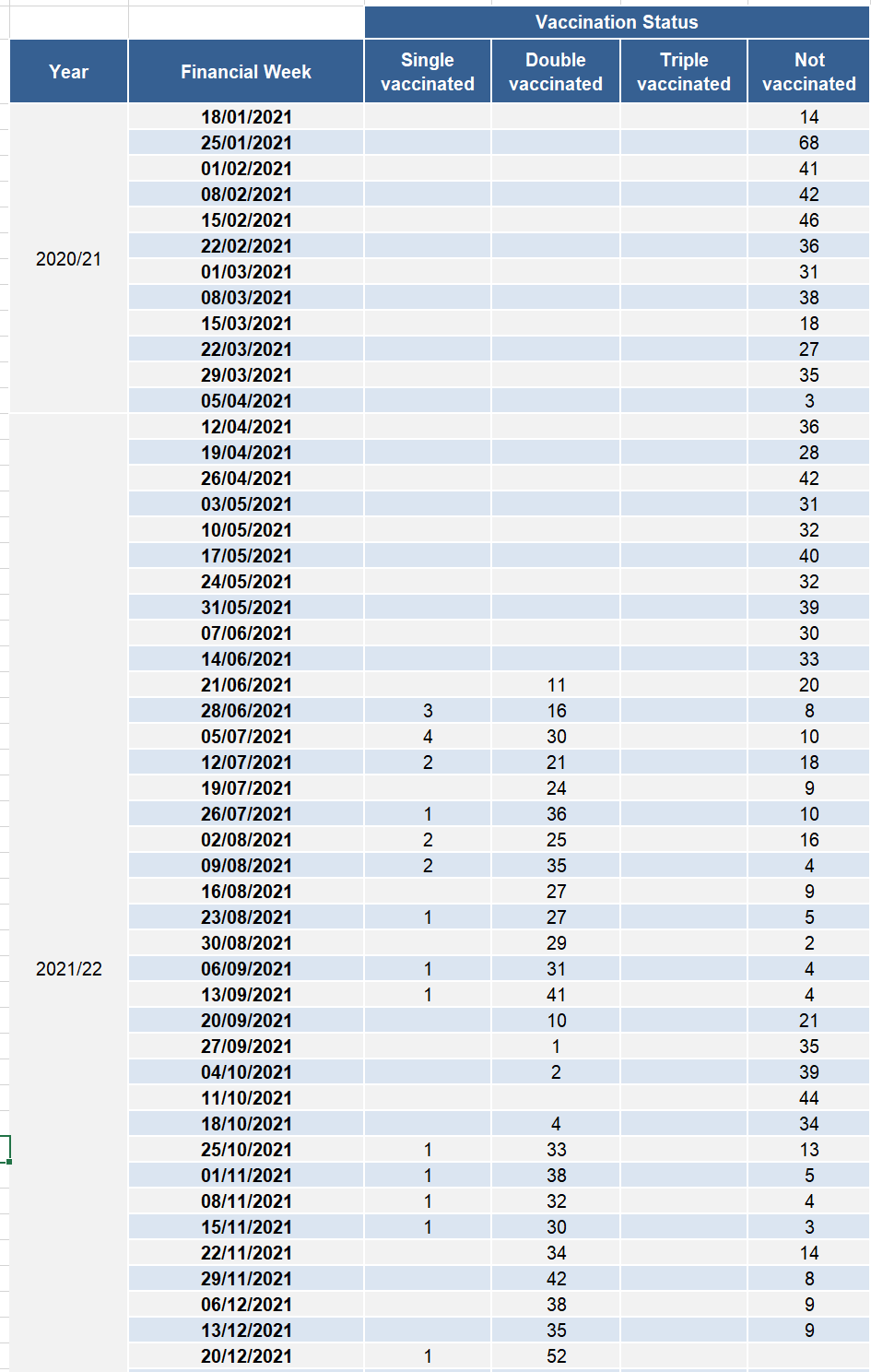
Conclusion
If Professor Fenton and his team are correct, claims of COVID-19 vaccinations being both safe and effective turn to dust before our eyes. They are not a miracle, but a magic trick: utterly compelling until the sleight of hand is revealed—then it’s impossible not to see. The examples given here are by no means exhaustive, Professor Fenton has also shown how statistical tricks such as survivor bias are employed to obscure vaccine dangers to pregnancy.59 His team’s work would also explain the unprecedented level of reports submitted to the US Vaccine Adverse Event Reporting System, and the UK Yellow Card System.
Zachary Stieber, a journalist at the Epoch Times, obtained data from the CDC via a Freedom of Information request. He reported that the CDC had ‘identified hundreds of safety signals for the two most widely administered COVID-19 vaccines’, and that ‘Bell’s palsy, blood clotting, and death were among the signals flagged through analyses of adverse event reports’.60
In the UK, Dr. Richard Ennos analysed the Yellow Card system and found it indicates ‘unequivocal safety signals’ for adverse reactions caused by the Pfizer and Moderna vaccines affecting the blood, the heart and female reproduction. He further concluded that the Medicines and Healthcare Products Regulatory Agency ‘has provided no protection to the U.K. public from the adverse effects of the novel COVID-19 vaccines’ and that it’s regular publication has ‘been an exercise in defending the COVID-19 vaccines from criticism rather than defending the U.K. public from the COVID-19 vaccines.’61
Questions for the State
This chapter has raised a number of challenges to the claims of safety and efficacy of the various COVID-19 vaccines—claims that were echoed by the state. In the light of this information, does the state stand by its position that the vaccines are both safe and effective?
If so, how would it account for the issues raised?
Five. Viral Origins
‘99 red balloons
Floating in the summer sky
Panic bells, it's red alert
There's something here from somewhere else
The war machine springs to life
Opens up one eager eye
Focusing it on the sky
The 99 red balloons go by’
Nena1
In this document so far we have examined the various policies that were mandated to stop the spread of COVID-19. We have questioned whether these mandates were effective, or whether they actually brought about the deaths they ostensibly sought to curb.
At some point it behoves us to ask, what is all of this based upon? What safety signal emerged from China at the turn of the decade that convinced the world a deadly virus was circulating?
Whilst there are reports of Chinese citizens becoming infected with COVID-19 in November of 2019,2 ‘patient zero’ is considered to have developed symptoms on the 1st of December.3 The first hospitalisation, retroactively confirmed to be a COVID-19 case, happened around a week after that.4
By the 31st of December, tests had been run to identify if a novel infectious agent was behind these cases. The Wuhan Municipal Health Commission released a briefing about early signs of a pneumonia outbreak in the city, which was picked up by various Chinese news agencies.5
In response to this, both Hong Kong and Taiwan tightened their inbound screening processes.6 This is also when the US CDC claims to have first learned of a ‘cluster of 27 cases of pneumonia’ in Wuhan.7 The following day, US CDC Director Robert Redfield was reportedly ‘rattled’, after being briefed about the severity of the virus.8 The United Nations then activated its ‘incident-management system’ and China reported the virus to the World Health Organization.9 The US CDC offered to send experts to assist the investigation.10 On the 3rd of January, the BBC reported on the ‘mysterious viral pneumonia which has infected dozens of people in the central city of Wuhan’.11
It was on this day that Chinese scientists claimed to have ruled out the possibility of various common respiratory pathogens, and identified the genetic sequence of three distinct strains of a novel coronavirus. This was confirmed as the cause of the viral pneumonia cluster on January 6th.12 The New York Times now reported on the outbreak.13 Chinese President Xi Jinping ‘made requests for the prevention and control work of the coronavirus outbreak’ at the Politburo of the Chinese Communist Party.14
All of this occurred without a single death being attributed to COVID-19.
This raises many questions—questions that were perhaps lost after the dramatic spikes in death rates around the world drew attention. Depending on where you draw the boundary, Wuhan is a city of approximately nine million people, comparable in population to New York. During the especially bad season of 2018, over 23 thousand New Yorkers were hospitalised with flu. At its peak there were over 18 thousand laboratory confirmed cases in one week.15 It’s reasonable to assume the death toll from this would have substantially contributed to the several thousand deaths the city sees during an average winter month.
At the point President Xi was taking steps to control the outbreak, the WHO and CDC were getting prepared, and the BBC and New York Times started reporting on it, there were a grand total of zero fatalities and 59 cases.16
At the risk of labouring the point, the graph below shows the excess mortality in Germany in March of 2018.17
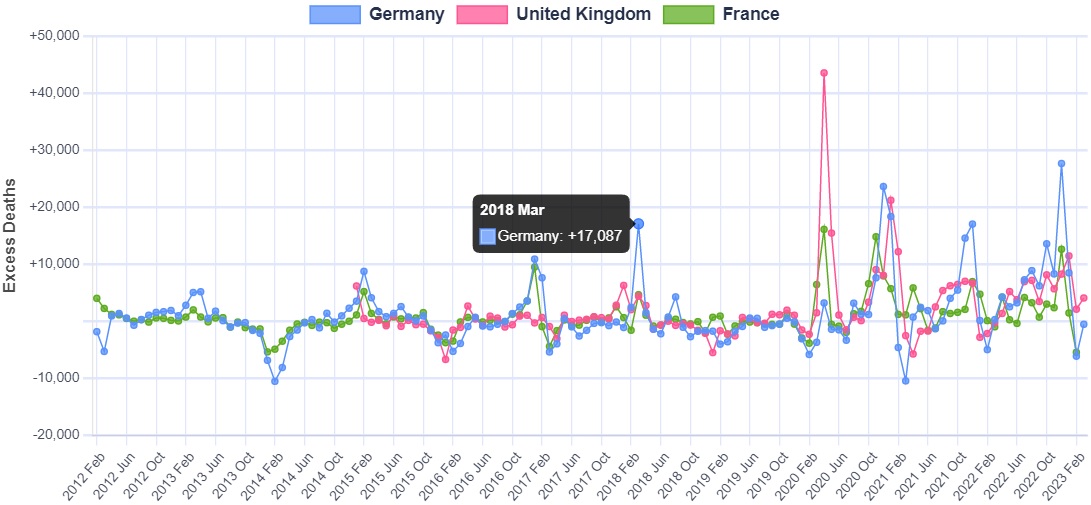
Somehow, Germany suffered an astounding 17,087 excess deaths in one single month. Yet, to the best of our knowledge, there is no sign that this caused international alarm. Markets were not closed down and disinfected, the CDC did not intervene, the international media did not run with the story. If a signal this strong does not draw the world’s attention, why was everyone so concerned about a disease that had zero deaths in China?
News reports from the time do not explain this. Initially, it might have been assumed that the Chinese were picking up on highly unusual symptoms. This may have seemed plausible, as not long after, stories appeared in the international media which implanted the idea of a highly unusual virus in the popular imagination.18
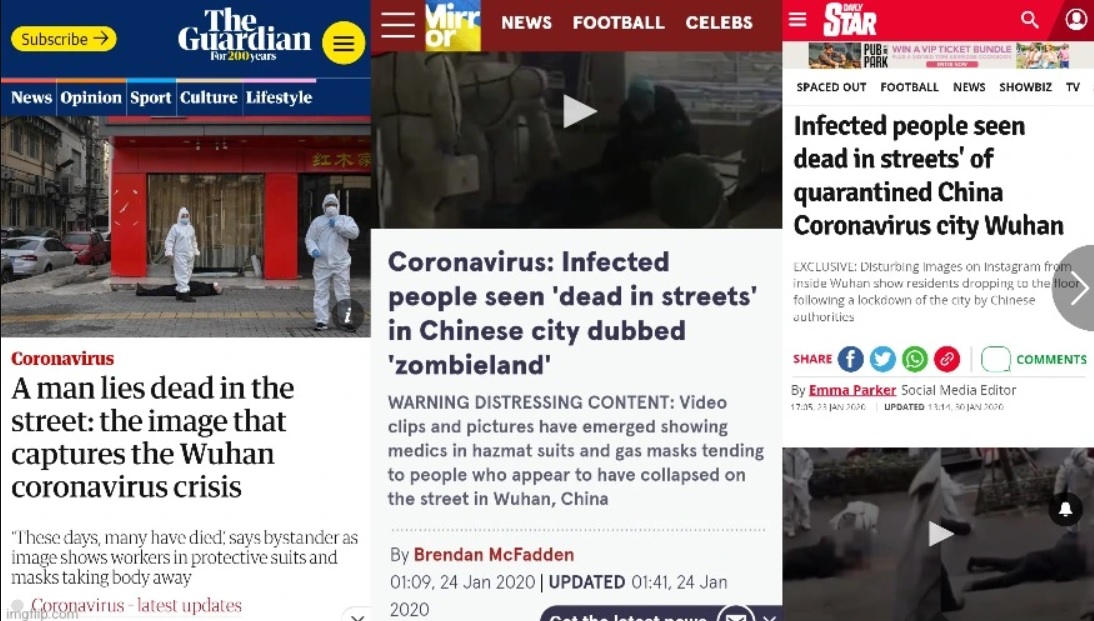
It soon became apparent however, that videos of people walking along the street then suddenly collapsing, were fake. In reality, and as the CDC confirms, COVID cannot be differentiated from the flu by symptoms alone:
‘You cannot tell the difference between flu and COVID-19 by the symptoms alone because they have some of the same signs and symptoms. Specific testing is needed to tell what the illness is and to confirm a diagnosis.’19
The question remains then, what did Chinese doctors observe that indicated the presence of a novel virus?
On the 3rd of January, Chinese scientists determined the genetic sequence of the virus they called COVID-19.20 Within two weeks, the WHO had published a test protocol capable of identifying this new virus.21
Everything that follows rests on these two pillars: that a novel virus was accurately identified, and that a polymerase chain reaction (PCR) test could accurately identify it. It was in the belief in the solidity of these pillars that countries around the world enacted mass testing and went into lockdowns. Both of these pillars involve complex science that the vast majority of people—including the media reporting on COVID and the politicians legislating for it—simply do not understand. At best, they have a very limited understanding, one that is reliant on chosen experts who they are unable to critique. If either of these pillars are flawed, the entire COVID narrative comes crashing down.
It is perhaps worth pausing for a moment to reflect that countries around the world took the most drastic cause of action, with the most incredibly far reaching consequences, based on science so few of us understand, and must essentially take on faith alone.
Amongst those who do understand it, this science is not without its critics. A team of twenty two scientists, led by molecular biologist Peter Borger, submitted a retraction request to the journal that published the original PCR protocol. They cited ‘numerous technical and scientific errors’, the most major of which was that the test was based on theoretical sequences of the virus, supplied by a laboratory in China, as none of the actual virus was available.22
Borger’s team also highlights the problem of cycle thresholds. PCR tests amplify genetic material, and if the level of amplification is to high, the result becomes meaningless:
‘In case of virus detection, >35 cycles only detects signals which do not correlate with infectious virus as determined by isolation in cell culture [reviewed in 2]; if someone is tested by PCR as positive when a threshold of 35 cycles or higher is used (as is the case in most laboratories in Europe & the US), the probability that said person is actually infected is less than 3%, the probability that said result is a false positive is 97%.’23
This is in line with comments made by the inventor of PCR, Dr. Kary Mullis, who said:
‘With PCR, if you do it well, you can find almost anything in anybody. It starts making you believe in the sort of Buddhist notion that everything is contained in everything else. If you can amplify one single molecule up to something which you can really measure, which PCR can do, then there’s just very few molecules that you don’t have at least one single one of them in your body, okay. So that could be thought of as a misuse of it, just to claim that it’s meaningful… PCR is just a process that’s used to make a whole lot of something out of something. That’s what it is. It doesn’t tell you that you’re sick and it doesn’t tell you that the thing you ended up with really was going to hurt you or anything like that.’24
As a substantial critique of the scientific underpinning of the PCR test is beyond the scope of this paper, more extensive resources are therefore provided in the endnotes.25
In addition to the scientific issues, there is also a purely mathematical problem with the accuracy of tests. If a test has a mere 1% false positive rate, it would seem like a person testing positive has a 99% chance of having the virus. Perhaps counter-intuitively, this is not the case, in fact the actual probability cannot be known without first knowing the prevalence of the virus in society.
As a thought experiment: imagine a society of 10 thousand people, where only 10 have contracted a certain virus. If everyone in this society took a 99% accurate test, the 10 infected would get positive results, but due to the 1% false positive rate, so would 100 uninfected people, making a total of 110. A person testing positive therefore has a 9.1% chance of actually being positive, not 99%. This obviously has damning implications for the use of PCR, given that the tests were used to stop people from leaving their homes etc.26
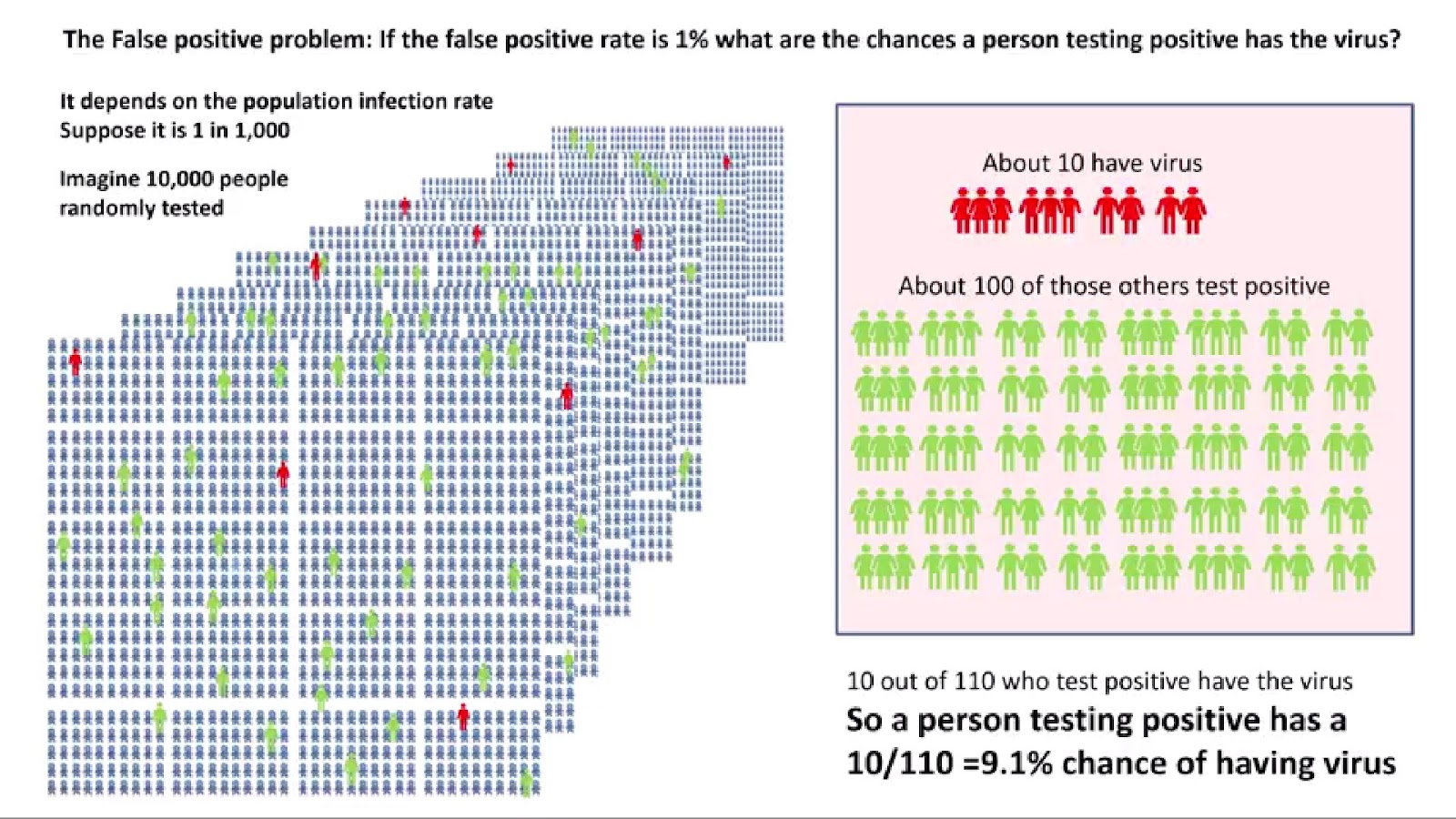
An example of what can go wrong with PCR occurred in 2006, in what The New York Times later described as the ‘epidemic that wasn’t’. This incident took place at the Dartmouth-Hitchcock Medical Center, in New Hampshire. It began when several healthcare workers developed a cough, and an infectious disease expert became concerned this signalled the beginning of a whooping cough epidemic. This was a concerning issue, as whooping cough would represent a serious threat to the hospital vulnerable patients. The New York Times reported that:
‘For months, nearly everyone involved thought the medical center had had a huge whooping cough outbreak, with extensive ramifications. Nearly 1,000 health care workers at the hospital in Lebanon, N.H., were given a preliminary test and furloughed from work until their results were in; 142 people, including Dr. Herndon, were told they appeared to have the disease; and thousands were given antibiotics and a vaccine for protection. Hospital beds were taken out of commission, including some in intensive care.
‘Then, about eight months later, health care workers were dumbfounded to receive an e-mail message from the hospital administration informing them that the whole thing was a false alarm.’27
Laboratory tests failed to confirm a single case of whooping cough. It appears the healthcare workers simply had ordinary respiratory diseases, such as the common cold. The outbreak of this pseudo-pandemic was attributed to placing too much faith in highly sensitive molecular tests. It is reasonable to assume that the furlonging of healthcare workers and reduction of hospital beds would have had real consequences on health outcomes.
Throughout the ages, human literature has warned of the perils of self-fulfilling prophecies. From the ancient Greek myth of Oedipus, through Shakespeare's Macbeth, to the modern myths of Harry Potter and Star Wars.28 Perhaps there is a reason for this beyond simply making a compelling story. The quotation from the start of this chapter is a verse from the song 99 Red Balloons. It tells the story of a nation mistaking these balloons for an enemy invasion, and readying its war machine. Seeing this, the suspected invader concludes it is under threat, and readies its own machine. The first nation takes this as confirmation that it was right all along, and war ensues.
The song reflects the sense of meaning the conflict brings. Lines like ‘This is what we've waited for, This is it boys, this is war’, illustrate how entire bureaucracies now find justification for their existence, whilst ‘Everyone's a superhero, Everyone's a Captain Kirk,’ speaks to how people are lifted out of the mundanity of life into a heroic narrative. It all ends in disaster however, as the singer is left ‘In this dust that was a city’, looking for a souvenir, ‘Just to prove the world was here’.
Has COVID-19 been such a ‘red balloon’? Has what happened at the Dartmouth-Hitchcock Medical Center simply played out on a global scale? Did we get into a vicious circle, where PCR tests were used to justify lockdowns, which caused a surge in excess deaths, which was taken as evidence that the tests were indeed right?
To repeat the conclusion of Chapter One: it is not within the scope of this document to draw grand conclusions to such questions. It is well within all of our scopes however, to assert that this remains the most centrally important question that we must all seek to answer.
Conclusion
‘It's quite possible that another virus comes along that's got a 10% mortality rate…Just imagine we had a virus that was selectively killing children because of their immune naivety. That is medically possible. If that happened, then all of these measures [emergency vaccines and lockdowns] could be completely justified… We could be in a situation where these things are actually completely necessary.’
Dr. John Campbell1
In 1958 Mao Tse-Tung initiated a campaign to eliminate all the sparrows from China. The reasoning ran that sparrows consumed grain, several pounds of it per bird per year, and this grain would be better used feeding the Chinese people.2
Millions of people collaborated to destroy nests, break eggs and shoot the birds from the sky. They would even bang pots and pans to prevent the sparrows from resting, causing them to drop dead from exhaustion. This may sound cruel, but as China had regularly suffered with famines throughout her history, grain provision was literally a matter of life or death for millions of people.
The plan was an overwhelming success, pushing the sparrow population to near extinction in China. This endeavour could be taken as a shining example of the necessity of state central planning. It would have been utterly futile for individual farmers to attempt to organise such a program themselves. Success depended on a top down, coordinated, authoritarian approach.
At least that’s how we might remember it, had it not gone so horribly wrong.
In addition to grain, sparrows eat locusts, and in their absence the insect population exploded. Locusts ravaged crops across China and contributed to perhaps the greatest famine in human history.
Mao’s ‘Great Leap Forward’ has become synonymous with hubris. It is the most cataclysmic example of communist ‘central’ planning. Such actions are not confined to communist states however, the United States use of DDT to eliminate mosquitoes also had horrendous unintended consequences.3
In the COVID-19 era we have heard much regarding the necessity of government action, often with criticism levied at governments who failed to take the bold and necessary steps to get the virus under control and save lives. This document has made the case that this is not true, that the actions of governments around the world were counterproductive, costing many lives whilst not demonstrably saving any.
The conflict that has arisen in society over approaches to COVID-19 could ultimately be thought of as a collision between two diametrically opposed worldviews. These worldviews have always existed in society, in perpetual conflict with each other, with COVID simply bringing it to a head.
The first view contends that certain challenges exceed society’s capacity to handle in a consensual, decentralised manner. A top down, centralised, authoritarian approach is required. One where people are told what to do and what is best for them by state appointed experts. Opinion contradicting these experts, irrespective of its source, is to be disregarded. Dissent is not to be tolerated. Refusal to go along with the chosen plans results in sanctions up to and include jail time.
This is the view that allowed New Zealand Prime Minister Jacinda Ardern to claim that her government would ‘continue to be your single source of truth’,4 or Dr. Anthony Fauci to declare an attack on him was an attack on science itself.5 It is the view that allowed a nasty aura to infect our societies, of recrimination for anyone not going along with the latest ‘science’, and for a moral self righteousness to take hold. We saw a rise of support for the kind of superstitious thinking that many of us felt had been discarded in the Middle Ages.6
The second view stands in complete contrast to this. It sees society as a complex, self organising system governed by economic laws as solid as the ones of physics. This approach emphasises pluralism, respect for individual rights and highlights the limits of knowledge and the need to experiment with many different approaches to complex problems. It recognises that the world does not stand still in order for us to measure it, but rather adapts in unpredictable ways to each intervention we make.
The 20th century saw a competition between these two worldviews play out. The Soviet Union and China embodied authoritarian central planning, whilst what we loosely call ‘the West’ embraced a more decentralised market based approach. For all the imperfections in the way it was embodied, the latter of these two ideologies overwhelmingly won out. Perhaps it did so however, only to then be discarded in favour of the former.
The reasons for the failure of ‘central’ planning are not a mystery: an authoritarian top down approach, which eschews pluralism in favour of ‘one size fits all’ thinking, can simply not hold up in the complexity of the world we encounter. A world where answers to complex problems are not obvious, where even the most intelligent people get stuck inside their own perspectives, unable to see another point of view.
States are not inherently virtuous incorruptible institutions that rise above the petty concerns of mere private citizens. They are just as subject to ideological capture as any other institution. They do not have a golden path to truth which makes them inherently more reliable. What they do have, is a limitless supply of funds and the ability to impose their will. This should not be conflated with wisdom.
The unprecedented cataclysm of the Four Pests Campaign did not cause the Chinese Communist Party to doubt the wisdom of authoritarian central planning. Instead, they concluded that they’d simply got the pest wrong, and swapped sparrows for bed bugs. As the quotation at the beginning of this chapter from Dr. John Campbell illustrates, there is a common sentiment that the underpinning philosophy of our approach to COVID-19 was correct, and only the application was wrong. In a future more deadly pandemic, such an approach may indeed be necessary. Beyond all criticism of the science and data, it is this philosophy we request justifies itself.
Let us take Dr. Campbell’s challenge: what if a virus came along that did kill one in ten people, or children, or one in ten children? Would authoritarian state central planning then be the best approach?
To say the least, it is simply not clear that this is the case. Mitigation efforts would themselves be dangerous, making an accurate estimation of viral dangers difficult. Vested interests would still seek to profit, by capturing state regulatory institutions and twisting the scientific underpinning of approaches. If no treatment presented itself, the situation could go on for a long time, the economic impacts would then also cost lives. It would therefore be better to allow society to self-organise around protecting the vulnerable. There would also be no way to compare different approaches and judge which gave the best results. Finally, it must be recognised that it is impossible to create a perfect world where no one dies. Pursuing such a utopia will invariably just lead to more death.
China’s cruel fate was not set in stone. In 1956, Mao Tse-Tung pursued a policy of letting ‘a hundred flowers bloom, and a hundred schools of thought contend.’ The following year it was revealed as a trap; with the dissidents now identified, Mao launched a harsh crackdown.
If a thousand flowers had bloomed in China, if decentralisation had been embraced, the country need not have experienced the horrors of famine, cultural revolution and persistent poverty for decades to come. What would have been the result of a thousand flowers blooming during COVID-19, if states had not mandated behaviour? It is clear we would have avoided the iatrogenic deaths, the pseudoscience of masking, the inhuman consequences and economic destruction of lockdowns and the harms of vaccines. We would also have avoided the divisiveness that crept into our societies, turning us against each other. As this document has attempted to demonstrate, it is not clear we would have suffered any ill consequences at all.
To revisit the Adam Curtis quotation that opened this essay then: it seems clear that not only can politicians not deliver dreams, neither can they protect us from nightmares. Their efforts to do so only make matters worse, taking what is essentially a fantasy and turning it into a real life horror. This essay is dedicated to those who seek to awaken from both dreams and nightmares, and meet the world as it is.
Endnotes
Introduction
1. The Power of Nightmares, BBC, Adam Curtis
One. Pandemic or Democide: What Caused the Excess Deaths?
1. How Many did Communist Regimes Murder?, by Rudolf Rummel
2. Weekly number of excess deaths in England and Wales from January 2020 to April 2023, Statista
3. Excess mortality during the Coronavirus pandemic (COVID-19), Our World in Data
4. Virus Mania: How the Medical Industry Continually Invents Epidemics, by Torsten Engelbrecht, Claus Köhnlein, MD, Dr. Samantha Bailey, MD and Dr. Stefano Scoglio
5. COVID-19 (excess) mortalities: viral cause impossible—drugs with key role in about 200,000 extra deaths in Europe and the US alone, By Torsten Engelbrecht, co-authored by Claus Köhnlein, MD, Real News Australia
6. Excess mortality during the Coronavirus pandemic (COVID-19), Our World in Data
7. Ibid
See also, In defence of alternative explanations for excess deaths other than a novel deadly virus spreading from Wuhan, Where are the Numbers?
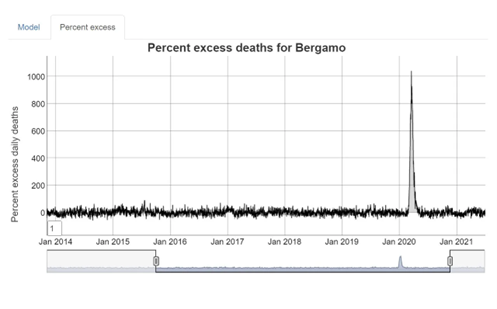
8. Excess mortality during the Coronavirus pandemic (COVID-19), Our World in Data
10. COVID-19 (excess) mortalities: viral cause impossible—drugs with key role in about 200,000 extra deaths in Europe and the US alone, By Torsten Engelbrecht, co-authored by Claus Köhnlein, MD, Real News Australia
11. Ibid
12. Ibid
13. All-cause mortality during COVID-19 - No plague and a likely signature of mass homicide by government response, Denis Rancourt
14. WHO Director-General's opening remarks at the media briefing on COVID-19
15. Critical preparedness, readiness and response actions for COVID-19, WHO. Please note: this document is the updated version from May 2021
16. Phylogenetic reconstruction of the initial stages of the spread of the SARS-CoV-2 virus in the Eurasian and American continents by analyzing genomic data, National Institute of Health
‘Results showed that the first cases of COVID-19 in the human population appeared in the period between July and November 2019 in China. The spread of the virus into other countries of the world began in the autumn of 2019. In mid-February 2020, the virus appeared in all the countries we analyzed.
‘In a short period of time, COVID-19 has spread from China to almost every country in the world (Chatterjee et al., 2020; Tabari et al., 2020). Media reports about the first cases of COVID-19 outside of China (other countries in Asia, Europe, America and Australia) became widespread in the second half of January 2020. On 30 January 2020, the World Health Organization (WHO) declared the COVID-19 outbreak as a global health emergency, and on 11 March 2020 it was declared as a worldwide pandemic. The problems of epidemiological studies of COVID-19 lie in the mass spread of asymptomatic and mild forms of the disease (Gao et al., 2020; (Zhao et al., 2020). Therefore, the early stages of the infection spread in the world, or in any country, could be hidden from epidemiologists.’
See also, Molecular evidence for SARS-CoV-2 in samples collected from patients with morbilliform eruptions since late 2019 in Lombardy, northern Italy, Environmental Research
And, SARS-CoV-2 was already spreading in France in late December 2019,
International Journal of Antimicrobial Agents
And, The presence of SARS-CoV-2 RNA in human sewage in Santa Catarina, Brazil, November 2019, Science of The Total Environment
And, The Compelling Evidence COVID-19 Was Spreading Across the U.S. in 2019 That Officials Are Ignoring, The Daily Sceptic
17. Ibid
Dr. Clare Craig proposes an explanation based on a ‘seasonal trigger’:
SAGE models need a reality check
See also, COVID-19 and Excess Deaths: A Defence of the Virus Theory, The Daily Sceptic, Will Jones
18. All-cause mortality during COVID-19 - No plague and a likely signature of mass homicide by government response, Denis Rancourt
Nature of the COVID-era public health disaster in the USA, from all-cause mortality and socio-geo-economic and climatic data, Denis Rancourt
19. Z-scores by country, Euromomo
20. Excess Mortality United States US Mortality
21. As if Expendable: The UK Government’s Failure to Protect Older People in Care Homes During the COVID-19 Pandemic, Amnesty International UK
22. Coronavirus: What's going wrong in Sweden's care homes?, BBC News
See also: Sweden's nursing home COVID failures haunt relatives left behind, Reuters
23. Coronavirus: Elderly people found 'dead and abandoned' at care homes in Spain, Sky News
See also: "We have not looked at the residences until they have been filled with the deceased" , Huffington Post
And: The impact of COVID-19 in nursing homes in Madrid, Spain: a need for assessment, The Lancet
24. Death stalks French nursing home, where corpses lie in rooms, Reuters
See also: As coronavirus creeps into French care homes, a 'tsunami' of deaths goes uncounted, France24
25. Did the Virus or Governments Kill More Canadians? A Statistical Analysis of Excess Deaths during the Pandemic, C2C Journal
See also: Who Killed Granny? Pandemic Death Protocols in Canada’s Long-term Care Facilities, C2C Journal
26. Cuomo nursing home order did cause more deaths, should’ve been reversed sooner: task force, New York Post
27. An Estimated 30,000 Americans Were Killed by Ventilators & Iatrogenesis in April 2020, Brownstone Institute, Michael Senger
See also: Dr. Jessica Hockett has written extensively on various aspects of the extreme excess mortality spike in New York: All Posts Related to New York City's Spring 2020 Mortality Event
28. Review of Liverpool Care Pathway for dying patients, An independent report for the UK Government
Liverpool Care Pathway: 'They told my family I was dying', BBC News
29. A Good Death? is available on Ickonic
See also: interview with Jacqui Deevoy
30. Euthanasia in the Pandemic?, Dr. John Campbell
31. COVID-19 rapid guideline: managing symptoms (including at the end of life) in the community, NICE guideline
32. Rapid Response: Managing COVID-19 symptoms in the community (including at the end of life): NICE NG163 is a welcome step, but needs review, The British Medical Journal
33. Comparison of graphs constructed by ‘Ben’ on Twitter, using data from Open Prescribing and Mortality Watch
It should be noted that the midazolam graph was limited to only show the use of the high end 10mg/2ml doses, to demonstrate they account for the vast majority. If all doses are taken into account the use is even higher:
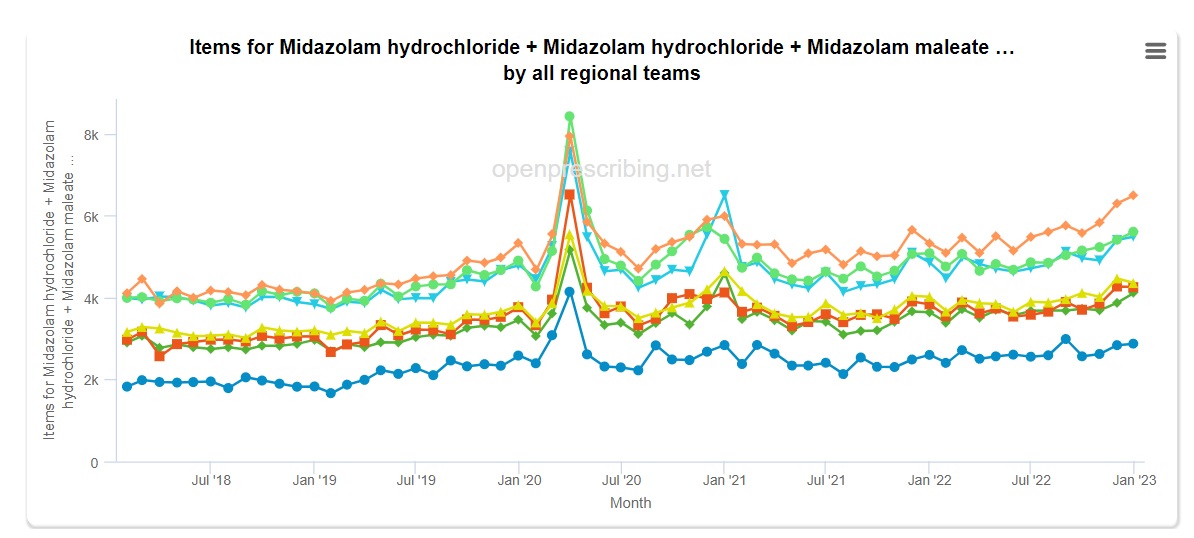
34. Levomepromazine and haloperidol data at Open Prescribing
Haloperidol safety at Drugs.com
‘Haloperidol may increase the risk of death in older adults with dementia-related psychosis and is not approved for this use.’
35. Midazolam in Italy, Dead Man Talking
And: Has Sweden’s controversial covid-19 strategy been successful?, The British Medical Journal
36. Europe has sanctioned euthanasia for the elderly ill with corona, Israel national News
37. Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness, The Journal of Infectious Diseases, Dr. Anthony Fauci
38. Comparison constructed from Open Prescribing and Mortality Watch data
See also: Antibiotic prescribing by GPs in England fell by 17% during the first 12 months of Covid without the usual winter increase, Antibiotic Research UK
The conclusion Antibiotic Research UK drew from this decrease was that it ‘hints at scale of over-prescribing in normal times’. That might be a fair conclusion to draw, had the fall not corresponded with a massive rise in the death rate
39. Outpatient antibiotic prescribing during the COVID-19 pandemic–United States, January 2019–October 2021, Cambridge University Press
40. Nature of the COVID-era public health disaster in the USA, from all-cause mortality and socio-geo-economic and climatic data, Dr. Denis Rancourt
41. Coronavirus: Five arrested in Isle of Man Abbotswood care home probe, BBC
42. Correspondence provided to the authors of this document by Mrs. Zandra Lewis. Printed with her permission.
Mrs. Lewis has been interviewed by the authors:
‘Nil by Mouth’, an Interview with Zandra Lewis on the COVID End of Life Pathways
Two. Mask Mandate
1. Dr. Anthony Fauci talks with Dr Jon LaPook about Covid-19, 60 Minutes, (March 2020)
Mask Mandate Efficacy
2. Masks: Before and After They Became Political, Brownstone Institute, Dr. Steve Templeton
3. Universal Masking in Hospitals in the Covid-19 Era, The New England Journal of Medicine (2020)
4. Nonpharmaceutical Measures for Pandemic Influenza in Nonhealthcare Settings—Personal Protective and Environmental Measures, Xiao et al. 2020. The Centers for Disease Control
5. Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza. World Health Organization
6. Masks may actually increase your coronavirus risk if worn improperly, surgeon general warns, CNN, 2020
7. Rational use of face masks in the COVID-19 pandemic, Feng et al. 2020. The Lancet
8. Facial Masking for Covid-19 — Potential for “Variolation” as We Await a Vaccine, Gandhi et al. 2020. The New England Journal of Medicine
9. CDC director says face masks may offer more protection against COVID than a vaccine. Here's what other experts say, CBS News
10. For a summary of the changing perspectives and politicisation of masks see The Brownstone Institute: Masks: Before and After They Became Political, by Professor Steve Templeton.
Further illustrative examples of the obvious politicisation of the CDC on masks can be found in Dr. Thomas Woods book, COVID Charts CNN Forgot. To take one example:
‘In early January 2021, the Centers for Disease Control published a Tweet that included this line, along with a link to an article about Delaware: “In Delaware, universal mask use helped reduce #COVID19 cases, hospitalizations, and deaths.”
‘Before I even show you Delaware’s chart, think about what it should look like if what this January 5 Tweet said weren’t misleading.
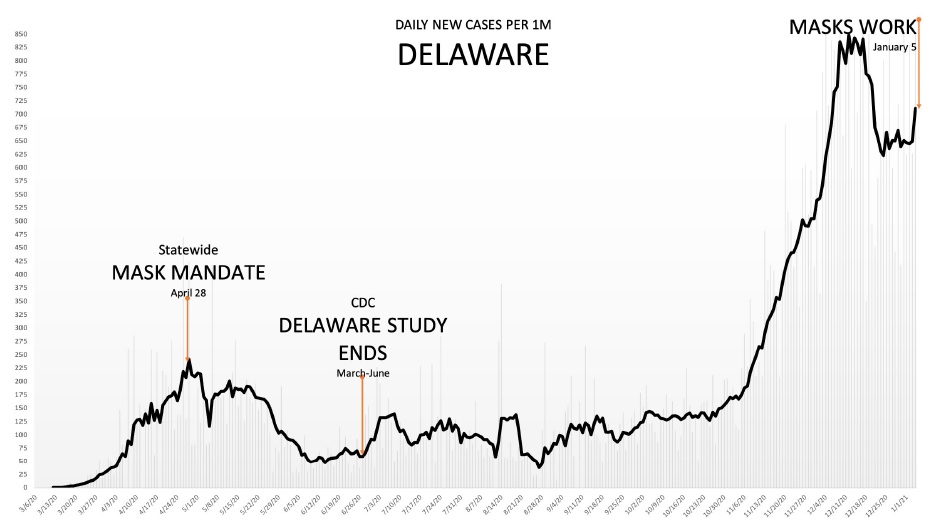
Source: Covid Tracking Project - 7 Day Avg. | Twitter: @ianmSC
‘Looking at these hospitalization numbers in January 2021, would your conclusion be: masks sure lowered the number of cases?
‘Are you not instead inclined to wonder: why on January 5 is the CDC Tweeting about the results of a study that concluded all the way back in June, and since which time hospitalizations have exploded even as mask usage has held steady or grown?’
11. For the studies against see More than 170 Comparative Studies and Articles on Mask Ineffectiveness and Harms, published at the Brownstone Institute by Dr. Paul Alexander. For studies for see the following footnote
12. For studies demonstrating mechanistic plausibility see: Potential utilities of mask‐wearing and instant hand hygiene for fighting SARS‐CoV‐2, Qing‐Xia Ma et al. 2020. National Library of Medicine
And: Testing the Efficacy of Homemade Masks: Would They Protect in an Influenza Pandemic? Anne Davies et al. 2013. National Library of Medicine
For evidence of demonstrably poor quality studies in support of masking see: Association Between K–12 School Mask Policies and School-Associated COVID-19 Outbreaks — Maricopa and Pima Counties, Arizona, July–August 2021, Megan Jehn et al. 2021. Centers for Disease Control and Prevention
And Dr. Vinay Prasad’s critique: Two New CDC Studies on Masking in School and Presentation
And:Effectiveness of Face Mask or Respirator Use in Indoor Public Settings for Prevention of SARS-CoV-2 Infection — California, February–December 2021 Kristin L. Andrejko et al. 2022. Centers for Disease Control and Prevention
And Dr. Vinay Prasad’s critique: Mask studies reach a new scientific low point and Presentation
And: School Masking Policies and Secondary SARS-CoV-2 Transmission, Angelique E. Boutzoukas et al. 2022. American Academy of Pediatrics
And Ian Miller’s critique at the Brownstone institute: CDC Promotes Another Misleading Mask Study
And Lifting Universal Masking in Schools — Covid-19 Incidence among Students and Staff, The New England Journal of Medicine
And Ian Miller’s critique: Boston School Masking Study is an Embarrassment to Science
13. Effectiveness of Adding a Mask Recommendation to Other Public Health Measures to Prevent SARS-CoV-2 Infection in Danish Mask Wearers, Henning Bundgaard et al. 2021. Annals of Internal Medicine
‘A total of 3030 participants were randomly assigned to the recommendation to wear masks, and 2994 were assigned to control; 4862 completed the study. Infection with SARS-CoV-2 occurred in 42 participants recommended masks (1.8%) and 53 control participants (2.1%)…Although the difference observed was not statistically significant, the 95% CIs are compatible with a 46% reduction to a 23% increase in infection.’
14. For a critique of DANMASK-19 see Of Masks and Methods, Thomas R. Frieden et al. 2021. Also published in the Annals of Internal Medicine
Also see Danish Study Doesn’t Prove Masks Don’t Work Against the Coronavirus, by Jessica McDonald at Factcheck.org
15. Impact of community masking on COVID-19: A cluster-randomized trial in Bangladesh, Jason Abaluck et al. 2021. Science
‘A randomized-trial of community-level mask promotion in rural Bangladesh during the COVID-19 pandemic shows that the intervention increased mask usage and reduced symptomatic SARS-CoV-2 infections, demonstrating that promoting community mask-wearing can improve public health.’
It is worth noting that the study did not find what it claims to have in its own conclusion. It did not find that ‘promoting community mask-wearing can improve public health’, it actually found no evidence that cloth masks are effective.
16. Re-analysis on the statistical sampling biases of a mask promotion trial in Bangladesh: a statistical replication, Maria Chikina et al. 2022
See also: The Bangladesh Mask Trial is re-analyzed and it falls apart, by Dr. Vinay Prasad. Dr. Prasad had originally been optimistic about the study
17. Physical interventions to interrupt or reduce the spread of acute respiratory viruses, Tom Jefferson et al. 2023. Cochrane Database of Systematic Reviews
18. On the Mask Study: An Interview with the Author, Maryanne Demasi, Brownstone Institute
19. Ibid
20. What the Cochrane Review Says About Masks For COVID-19 — and What It Doesn’t, FactCheck.org
21. Masks: Before and After They Became Political, Brownstone Institute, Dr. Steve Templeton
And More Evidence from the UK that Masks Don’t Work, Brownstone Institute, Ian Miller
And COVID Charts CNN Forgot, Dr. Thomas Woods
Mask mandate harms
22. Rapid Response: Covid-19: important potential side effects of wearing face masks that we should bear in mind, Dr. Antonio Lazzarino. British Medical Journal, 2020,
23. An extensive summary of mask related harms has been composed for the Brownstone Institute by epidemiologist Dr. Paul Alexander: More than 170 Comparative Studies and Articles on Mask Ineffectiveness and Harms
See also the recently published meta-study: Physio-metabolic and clinical consequences of wearing face masks—Systematic review with meta-analysis and comprehensive evaluation, Kai Kisielinski et al. 2023. Frontiers in Public Health
Masks restrict breathing and increase levels of carbon dioxide
24. Open letter from medical doctors and health professionals to all Belgian authorities and all Belgian media, Docs 4 Open Debate
25. Physio-metabolic and clinical consequences of wearing face masks—Systematic review with meta-analysis and comprehensive evaluation, Kai Kisielinski et al. 2023. Frontiers in Public Health
‘Masks interfered with O2-uptake and CO2-release and compromised respiratory compensation. Though evaluated wearing durations are shorter than daily/prolonged use, outcomes independently validate mask-induced exhaustion-syndrome (MIES) and down-stream physio-metabolic dysfunctions. MIES can have long-term clinical consequences, especially for vulnerable groups. So far, several mask related symptoms may have been misinterpreted as long COVID-19 symptoms. In any case, the possible MIES contrasts with the WHO definition of health.’
And: A German study collected parent’s reports of over twenty five thousand children’s experiences wearing masks. Impairments caused by wearing the mask were reported by 68% of the parents. These included irritability (60%), headache (53%), difficulty concentrating (50%), less happiness (49%), reluctance to go to school/kindergarten (44%), malaise (42%) impaired learning (38%) and drowsiness or fatigue (37%).
Corona child studies "Co-Ki": first results of a Germany-wide register for covering the mouth and nose (mask) in children, Schwarz et al. 2021 Monthly paediatrics Journal of Pediatrics and Adolescent Medicine
And: A French study found wearing a surgical mask significantly increased dyspnea (shortness of breath) during a six minute walk.
Effect of a surgical mask on six minute walking distance Pearson et al. 2017
And: A study by the Leipzig University Hospital used a stationary bicycle and treadmill to show masks cause measurably impairment of breathing:
‘The subjects were examined without a mask, with surgical masks and with FFP2 masks. The masks therefore affect breathing, especially the volume and the highest possible speed of the air when exhaling. The maximum possible force on the ergometer was significantly reduced.’
‘A faster acidification of the blood during exertion was registered in the metabolism. The participants also used questionnaires to assess their subjective feelings, which also showed a significant impairment of well-being.’
Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity Clinical Research in Cardiology (6.7.2020). See summary in Science
‘The literature revealed relevant adverse effects of masks in numerous disciplines. In this paper, we refer to the psychological and physical deterioration as well as multiple symptoms described because of their consistent, recurrent and uniform presentation from different disciplines as a Mask-Induced Exhaustion Syndrome (MIES). We objectified evaluation evidenced changes in respiratory physiology of mask wearers with significant correlation of O2 drop and fatigue (p < 0.05), a clustered co-occurrence of respiratory impairment and O2 drop (67%), N95 mask and CO2 rise (82%), N95 mask and O2 drop (72%), N95 mask and headache (60%), respiratory impairment and temperature rise (88%), but also temperature rise and moisture (100%) under the masks. Extended mask-wearing by the general population could lead to relevant effects and consequences in many medical fields.’
‘Here are the pathophysiological changes and subjective complaints: 1) Increase in blood carbon dioxide 2) Increase in breathing resistance 3) Decrease in blood oxygen saturation 4) Increase in heart rate 5) Decrease in cardiopulmonary capacity 6) Feeling of exhaustion 7) Increase in respiratory rate 8) Difficulty breathing and shortness of breath 9) Headache 10) Dizziness 11) Feeling of dampness and heat 12) Drowsiness (qualitative neurological deficits) 13) Decrease in empathy perception 14) Impaired skin barrier function with acne, itching and skin lesions’
And: Preliminary report on surgical mask induced deoxygenation during major surgery
‘Considering our findings, pulse rates of the surgeon's increase and SpO2 decrease after the first hour. This early change in SpO2 may be either due to the facial mask or the operational stress. Since a very small decrease in saturation at this level, reflects a large decrease in PaO2, our findings may have a clinical value for the health workers and the surgeons.’
And: Carbon dioxide re-breathing with close fitting face respirator masks
‘A healthy intensivist (SF), wearing such a respirator (Tecnol Fluidshield PFR95, Kimberly Clark Corporation, Roswell, GA) to perform a percutaneous tracheostomy on a patient with multidrug resistant pulmonary tuberculosis, experienced dyspnoea, tachycardia and tremor after 30min. End-tidal carbon dioxide measured at the mouth by hand-held capnometry was 6.3kPa (normal value 5.3 kPa). We postulated that the symptoms were due to hypercapnia.’
And: Effect of a surgical mask on six minute walking distance, National Institute of Health
‘Distance was not modified by the mask (P=0.99). Dyspnea variation was significantly higher with surgical mask (+5.6 vs. +4.6; P<0.001) and the difference was clinically relevant. No difference was found for the variation of other parameters. Wearing a surgical mask modifies significantly and clinically dyspnea without influencing walked distance.’
‘Since COVID-19 outbreak, 42/46 (91.3%) of respondents with pre-existing headache diagnosis either "agreed" or "strongly agreed" that the increased PPE usage had affected the control of their background headaches, which affected their level of work performance.’
26. Cutting Edge: Hypoxia-Inducible Factor 1 Negatively Regulates Th1 Function
‘Our data demonstrate that Th1 cells [cells that support the immune system] lose their capacity to produce IFN-γ when cultured under hypoxia.’
‘Our data indicate that oxygen availability can function as a local modulator of CD4+ T cell responses and thus influences tumour immune surveillance in inflammation-associated colon cancer.’
And: Hypoxia-driven immunosuppression contributes to the pre-metastatic niche
‘Primary tumor cells create favorable microenvironments in secondary organs, termed pre-metastatic niches, that promote the formation of metastases. Using immune competent syngenic breast cancer mouse models, we have recently demonstrated that factors secreted by hypoxic tumor cells condition pre-metastatic niches by recruiting CD11b+/Ly6Cmed/Ly6G+ myeloid cells and suppressing natural killer cell functions.’
And: Chronic intermittent hypoxia induces atherosclerosis
‘Nine of 10 mice simultaneously exposed to Chronic intermittent hypoxia [CIH] and high-cholesterol diet developed atherosclerotic lesions in the aortic origin and descending aorta. In contrast, atherosclerosis was not observed in mice exposed to intermittent air and a high-cholesterol diet or in mice exposed to CIH and a regular diet…CIH causes atherosclerosis in the presence of diet-induced dyslipidemia.’
And: Face Masks Pose Serious Risks To The Healthy, Dr. Russell Blaylock
‘The importance of these findings is that a drop in oxygen levels (hypoxia) is associated with an impairment in immunity. Studies have shown that hypoxia can inhibit the type of main immune cells used to fight viral infections called the CD4+ T-lymphocyte. This occurs because the hypoxia increases the level of a compound called hypoxia inducible factor-1 (HIF-1), which inhibits T-lymphocytes and stimulates a powerful immune inhibitor cell called the Tregs. This sets the stage for contracting any infection, including COVID-19 and making the consequences of that infection much graver. In essence, your mask may very well put you at an increased risk of infections and if so, having a much worse outcome.
‘People with cancer, especially if the cancer has spread, will be at a further risk from prolonged hypoxia as the cancer grows best in a microenvironment that is low in oxygen. Low oxygen also promotes inflammation which can promote the growth, invasion and spread of cancers. Repeated episodes of hypoxia has been proposed as a significant factor in atherosclerosis and hence increases all cardiovascular (heart attacks) and cerebrovascular (strokes) diseases.
27. Effect of Face Masks on Gas Exchange in Healthy Persons and Patients with Chronic Obstructive Pulmonary Disease, Michael Campos et al. 2020. Annals of the American Thoracic Society
28. Physio-metabolic and clinical consequences of wearing face masks—Systematic review with meta-analysis and comprehensive evaluation, Kai Kisielinski et al. 2023. Frontiers in Public Health
Just prior to publication of this document, the study was retracted by the publishing journal, who issued the following statement:
‘Following publication, concerns were raised regarding the scientific validity of the article. An investigation was conducted in accordance with Frontiers’ policies. It was found that the complaints were valid and that the article does not meet the standards of editorial and scientific soundness for Frontiers in Public Health; therefore, the article has been retracted. This retraction was approved by the Chief Editors of Frontiers in Public Health and the Chief Executive Editor of Frontiers. The authors did not agree to this retraction.’
Whether the retraction is due to genuine scientific errors, or has been made for more political reasons remains to be seen. With this noted, we have therefore kept the reference.
Masks are a breeding ground for bacteria
29. Masks and Coronavirus Disease 2019 (COVID-19), Angel N. Desai et al. 2020. JAMA
30. Contamination by respiratory viruses on outer surface of medical masks used by hospital healthcare workers, BMC Infectious Diseases:
‘Respiratory pathogens on the outer surface of the used medical masks may result in self-contamination. The risk is higher with longer duration of mask use (> 6 h) and with higher rates of clinical contact. Protocols on duration of mask use should specify a maximum time of continuous use, and should consider guidance in high contact settings.’
Physio-metabolic and clinical consequences of wearing face masks—Systematic review with meta-analysis and comprehensive evaluation, Kai Kisielinski et al. 2023. Frontiers in Public Health:
‘Together with the immune-inhibiting mechanisms mentioned above, we found some other possible deleterious mask effects that impede healthy natural breathing. The most prominent and extreme effect was found in the increase of air humidity and skin temperature within the dead space of the mask (Figures 5, 9B). Increased humidity and temperature can increase droplet and aerosol generation, which facilitate liquid penetration through the mask mesh. This not only increases the chance of microorganism (fungal and bacterial pathogens) growth on and in masks (134–136) causing increased risk for accumulation of fungal and bacterial pathogens (134, 136) including mucormycosis (137), but also leading to re-breathing of viruses that may be trapped and enriched within the moisturized mask meshwork.’
Surgical masks as source of bacterial contamination during operative procedures, Journal of Orthopaedic Translation
‘The bacterial count on the surface of SMs increased with extended operating times; significant difference was found between the 4- to 6-hour and 0-hour groups (p < 0.05). When we analysed the bacterial counts from the same surgeon, a significant increase was noted in the 2-hours group. Moreover, the bacterial counts were significantly higher among the surgeons than the OR. Additionally, the bacterial count of the external surface of the second mask was significantly higher than that of the first one.’
Your corona mask really is that scary, Blick Business. An article on mask tests run by the German consumer magazine K-Tipp.
‘The result is sobering. The masks are full of bacteria and mold. The reason: Masks act like filters, the breathing air flows through the fibers of the fabric. This has consequences: bacteria and fungi get stuck. They multiply rapidly in the warm, humid mask environment.’
The adverse effects of masking on the skin have also been studied:
The adverse skin reactions of health care workers using personal protective equipment for COVID-19, National Library of Medicine
‘The most common adverse skin reactions among HCWs wearing N95 masks were nasal bridge scarring (68.9%) and facial itching (27.9%). The most common adverse skin reactions among HCWs wearing latex gloves were dry skin (55.7%), itching (31.2%), and rash (23.0%). The most common adverse skin reactions among HCWs wearing protective clothing were dry skin (36.1%) and itching (34.4%).When most HCWs wear PPE for a long period of time, they will experience adverse skin reactions. The incidence of adverse skin reactions to the N95 mask was 95.1%, that to latex gloves was 88.5%, and that to protective clothing was 60.7%.’
“The duration of wearing masks showed a significant impact on the prevalence of symptoms (p < 0.001). Type IV hypersensitivity was significantly more likely in participants with symptoms compared to those without symptoms (p = 0.001), whereas no increase in symptoms was observed in participants with atopic diathesis. HCWs used facial skin care products significantly more often than non-HCWs (p = 0.001).
And dental effects have been observed: ‘Mask mouth’ is a seriously stinky side effect of wearing masks, New York Post
31. Dangerous pathogens found on children’s face masks, Rational Ground
‘A group of parents in Gainesville, FL, sent 6 face masks to a lab at the University of Florida, requesting an analysis of contaminants found on the masks after they had been worn. The resulting report found that five masks were contaminated with bacteria, parasites, and fungi, including three with dangerous pathogenic and pneumonia-causing bacteria.’
See also: Mask Report from Florida University
And: Amanda Donoho being interviewed on FOX News
32. Predominant Role of Bacterial Pneumonia as a Cause of Death in Pandemic Influenza: Implications for Pandemic Influenza Preparedness, The Journal of Infectious Diseases, Dr. Anthony Fauci
Masks and all cause mortality
33. The Foegen effect: A mechanism by which facemasks contribute to the COVID-19 case fatality rate, Fögen, Zacharias MD (2022). Medicine
Masks cause viruses to be re-inhaled
34. Ibid
‘Chan et al proved the “Foegen effect” in a golden Syrian hamster by showing a significant increase in viral load in the lungs of masked hamsters compared with non-masked hamsters (P < .05).’
Masks are composed of chemicals which can be toxic
35. Potentially toxic masks distributed in schools and daycares in Quebec, CBC News
And: Health Canada issues advisory for disposable masks with graphene, CBC News
36. Titanium dioxide particles frequently present in face masks intended for general use require regulatory control, Nature
‘Although titanium dioxide (TiO2) is a suspected human carcinogen when inhaled, fiber-grade TiO2 (nano)particles were demonstrated in synthetic textile fibers of face masks intended for the general public.’
And: COVID-19: Performance study of microplastic inhalation risk posed by wearing masks, Journal of Hazardous Materials
‘The inhalation risk posed by spherical- and fiber-like microplastics was high regardless of with or without wearing a mask. N95 exhibited good performance in reducing spherical- and fiber-like microplastic inhalation compared with the other masks and no mask even after undergoing different disinfection treatments. For masks without treatment used for 720 h, spherical-type microplastic inhalation risk continuously decreased compared with not wearing a mask. Meanwhile, fiber-like microplastic inhalation risk increased, except for N95. All the investigated disinfection processes led to varying extents of microplastic inner structure damage, increasing the risk of microplastic inhalation. Nonetheless, the use of masks is crucial during the pandemic scenario even though they might contribute some microplastics inhalation, it is minor problem as compared with protecting humans from COVID-19.’
The limitations of knowledge on this topic was acknowledged in the recent meta-study:
‘Our systematic review rarely discussed the inhaled toxins associated with the mask. Inhalation and ingestion of toxic substances, which are ingredients of the masks, are also of importance in evaluating this pandemic non-pharmaceutical intervention (NPI).’
Physio-metabolic and clinical consequences of wearing face masks—Systematic review with meta-analysis and comprehensive evaluation, Kai Kisielinski et al. 2023. Frontiers in Public Health
37. Coronavirus face masks: an environmental disaster that might last generations
Mask Mandates and Risk Compensation
38. Risk Compensation is also known as the Peltzman Effect, after economist Dr. Sam Peltzman who first studied this phenomenon.
The Effects of Automobile Safety Regulation, Journal of Political Economy
An anecdote from economist Dr. David Henderson’s article, What the Peltzman Effect Is and Isn't, is instructive:
‘In the early 1990s, my wife, daughter, and I were driving at the start of a vacation. I was driving my wife’s 1990 Camry wagon at about 65 to 70 mph in a 65 mph zone. My daughter, who was about 7, was sitting in the back. She realized that she had packed a book she wanted to read in a suitcase in the trunk. If she were to unlock her seatbelt, she could reach back and get it. She asked permission to do so. My wife and I consulted briefly and decided that she could but that I should drive “less intensely.” So I slowed to 55 mph and looked around even more hawkishly than was my wont.’
39. For criticism see: Risk Compensation: Revisited and Rebutted, Professor Barry Pless
And: Our Worst Idea About “Safety”, article at Slate, by Tim Requarth
And: Face coverings do not lead to false sense of security, existing evidence suggests, Science Daily
For more favourable accounts see: Masks, Seatbelts, and Peltzman Effects, article at the American Institute for Economic Research by Vincent Geloso
And: Do Face Masks Create a False Sense of Security? A COVID-19 Dilemma, Med Rxiv (not peer reviewed)
‘We find face mask mandates lead people to spend 20-30 minutes less time at home per day. We find face mask mandates increase trip taking to a variety of locations, chief among them are restaurants. This substitution behavior is concerning given the limited information on the protective value of casual face coverings.’
40. Masks, Seatbelts, and Peltzman Effects, article at the American Institute for Economic Research, by Vincent Geloso
41. It could be argued that masks act as a visual reminder to socially distance. This was of course not the reason given for mandating them however, if a visual symbol was thought to be a good idea then mandating one that did not come with promised health benefits would have been preferable.
42. A Partial List of the Myriad Abuses That Facemasks Inflict on Our Children, Aaron Hertzberg, Brownstone Institute
A particularly egregious account of the common experience of benign required to make medical information public can be found in Laura Dodsworth’s article, Masks Did Not Do Nothing; They Wrought Havoc:
‘I have several disabilities, physical and psychological. I am unable to wear a face mask because I have PTSD from sexual trauma as a young teen. I’m sorry for TMI but it’s relevant. I was raped and penetrated in my mouth too. Due to this, nothing can cover my mouth, it’s an instant panic attack.
I had to attend the minor injuries unit at hospital yesterday. When I approached the desk to book in, I was instantly ordered to put on a mask. One was offered to me, and I replied I was unable to do so due to a mental health condition. The receptionist fetched a nurse who asked why I was refusing to wear one and said that if I did not, then I would be removed from the unit. This area is very open and very public, with other patients being seen at the side of me. I asked for a private area, and this was refused. I was also wearing a sunflower lanyard.
‘I was becoming extremely anxious at this point and explained that I have PTSD. They wanted details. I was essentially railroaded into detailing what happened as a teen. I was told to wait and then taken into a room with a doctor and another nurse. I again had to explain in detail my PTSD. I was then offered a visor type mask which I found very claustrophobic and in all honesty unbearable, but was left in no doubt non-compliance would lead to my being asked to leave.
‘I was then triaged, assessed and treated. In total I explained everything three times. I had an hour-long major panic attack in the car afterwards. I had two more overnight. Since then I have been very on edge and I can’t sleep.’
Four. Lockdowns
1. Deaths Soar In Country That Didn’t Lock Down, CNN
2. Former United Nations Assistant Secretary-General, Ramesh Thakur, has written an retrospective account of predicted lockdown harms: Governments Were Given Credible Warnings about Lockdown Harms but Didn’t Listen
3. Coronavirus: World risks 'biblical' famines due to pandemic - UN, BBC News
And: U.N. warns economic downturn could kill hundreds of thousands of children in 2020, Reuters
4. Virus could push half a billion people into poverty, BBC News
5. Untold story of lockdown: sharp surge in child trafficking, The Indian Express
6. Why most Covid-19 deaths won’t be from the virus, BBC Future
7. If this goes on for six months, 50,000 more people could die of cancer, Daily Mail
8. As if Expendable: The UK Government’s Failure to Protect Older People in Care Homes During the COVID-19 Pandemic, Amnesty International UK
9. Non-pharmaceutical public health measures for mitigating the risk and impact of epidemic and pandemic influenza, World Health Organization
It has been objected that this WHO document refers to influenza pandemics, not coronavirus ones. It is not clear however, why this would change the recommendations, and why policies that are considered ineffective for the former would be effective for the latter.
The WHO position is consistent with that of the UK Department of Health from 2011, UK Influenza Pandemic Preparedness Strategy 2011
See also, What They Said about Lockdowns before 2020, American Institute for Economic Research
10. China’s smog city: What Wuhan looks like with 20 times the U.S. dust limit, Grist
11. China Wants Activists to Stay Out of Its War on Pollution, Bloomberg
And, China has made major progress on air pollution. Wuhan protests show there’s still a long way to go, CNN
12. ‘Polluted air’ could be an important cause of Wuhan pneumonia, Capital Cambodia
13. How Phony Coronavirus “Fear Videos” Were Used as Psychological Weapons to Bring America to Her Knees, Revolver
14. China is being "quite transparent," says NIH head, CNN
15. China extended its Wuhan coronavirus quarantine to 2 more cities, cutting off 19 million people in an unprecedented effort to stop the outbreak, Business Insider
16. How Covid Lockdowns Came to Italy, The New Normal, Michael Senger
17. Implementation Programme of the Plan of Action on Health Cooperation, The Ministry of Health of the Italian Republic
18. A Health Action Plan has Been Linking Italy to China for Twenty Years, Nuovo Giornale Nazionale
19. Board of Directors, Silk Roads Cities Alliance
20. Italy declares coronavirus emergency after first two cases confirmed, Reuters
21. Italians struggle with 'surreal' lockdown as coronavirus cases rise, The Guardian
22. Italy 2020: Inside Covid’s ‘Ground Zero’ in Europe, Michael Bryant, 21st Century Wire
And, The Lombardy Analysis, Jonathan Engler
And, Were the unprecedented excess deaths curves in Northern Italy in spring 2020 caused by the spread of a novel deadly virus?, Jonathan Engler
23. Hope. A right name for Healthcare. The most left-wing health minister in history, the defense of the NHS and the solution to the serious shortages of doctors, SIVeMP Veneto
24. Hope in the never-released book: "Thus the pandemic will help the left", Oltre la Linea
See also, Roberto Speranza said...:"Because we will heal"... all the lies and omissions in the book that the Minister sent to the pulp, Alfonso Guizzardi
And, Covid, Speranza postpones the sale of her book on the pandemic, la Repubblica
25. The Dragnet in Lombardy, Italy: Patient Zero of Lockdowns, The New Normal, Michael Senger
26. Ibid
27. Ibid
28. The 55 pages with shock scenarios in the government's secret plan, L Giornale
29. The Dragnet in Lombardy, Italy: Patient Zero of Lockdowns, The New Normal, Michael Senger
30. Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV), World Health Organization
31. WATCH: Chinese stormtroopers are welding doors shut on buildings so people can't even get out when their homes catch on fire, Not the Bee
32. What’s Behind The WHO’s Lockdown Mixed-Messaging, American Institute for Economic Research
33. Twitter account of Dr. Tedros Adhanom Ghebreyesus
34. Press Conference of WHO-China Joint Mission on COVID-19, World Health Organization
35. For a history of lockdown science and ideology see: The REAL Story of the Birth of ‘Social Distancing’ — the Western Term for Lockdown, The New Normal, Michael Senger
36. Suppression of COVID-19 outbreak in the municipality of Vo’, Italy, MedRxiv, Neil Ferguson et al.
37. The Earliest Days of the Italian Pandemic, or: Why Nobody Wants To Talk About February 2020 Anymore, eugyppius: a plague chronicle
38. The Dragnet in Lombardy, Italy: Patient Zero of Lockdowns, The New Normal, Michael Senger
39. Neil Ferguson interview: China changed what was possible, UnHerd
40. How Phony Coronavirus “Fear Videos” Were Used as Psychological Weapons to Bring America to Her Knees, Revolver
41. Silent Invasion: The Untold Story of the Trump Administration, Covid-19, and Preventing the Next Pandemic Before It's Too Late, Dr. Deborah Birx
See also, Deborah Birx’s “Silent Invasion”: a Guide to Destroying America From Within, The New Normal, Michael Senger
42. Ibid
43. The REAL Story of the Birth of ‘Social Distancing’ — the Western Term for Lockdown, The New Normal, Michael Senger
44. Governments Were Given Credible Warnings about Lockdown Harms but Didn’t Listen, Former United Nations Assistant Secretary-General Ramesh Thakur
45. The Masked Ball of Cowardice, Michael Senger
Lockdown efficacy
46. What We’ve Learned About So-Called ‘Lockdowns’ and the COVID-19 Pandemic, Factcheck.org
47. Molecular evidence for SARS-CoV-2 in samples collected from patients with morbilliform eruptions since late 2019 in Lombardy, northern Italy, Environmental Research
‘The first sample that tested positive for SARS-CoV-2 RNA was a urine sample collected as early as September 12th, 2019, from an 8-months old child whose serum was also IgG and IgM positive’
See also, Phylogenetic reconstruction of the initial stages of the spread of the SARS-CoV-2 virus in the Eurasian and American continents by analyzing genomic data, National Institute of Health
And, SARS-CoV-2 was already spreading in France in late December 2019,
International Journal of Antimicrobial Agents
And, The presence of SARS-CoV-2 RNA in human sewage in Santa Catarina, Brazil, November 2019, Science of The Total Environment
And, The Compelling Evidence COVID-19 Was Spreading Across the U.S. in 2019 That Officials Are Ignoring, The Daily Sceptic
The line for Italy has been inserted at the start of the regional Lombardy lockdown, not the later national one. This is justified as the deaths were disproportionately located in the Lombardy region.
See, The Lombardy Analysis, Jonathan Engler
And, Were the unprecedented excess deaths curves in Northern Italy in spring 2020 caused by the spread of a novel deadly virus?, Jonathan Engler
50. Fauci defends coronavirus lockdowns as saving ‘millions of lives’, The Hill
51. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe, Nature
‘We find that across 11 countries 3.1 (2.8–3.5) million deaths have been averted owing to interventions since the beginning of the epidemic; Extended Data Fig. 5 compares the actual total deaths to the counterfactual total deaths. The counterfactual model without interventions is illustrative only, and reflects the assumptions of our model. We do not account for changes in behaviour; in reality, even in the absence of government interventions we would expect Rt to decrease and therefore would overestimate deaths in the no-intervention model.’
See also, Inferring change points in the spread of COVID-19 reveals the effectiveness of interventions, National Center for Biotechnology Information
Lockdown timing and efficacy in controlling COVID-19 using mobile phone tracking, The Lancet
The Efficacy of Lockdown Against COVID-19: A Cross-Country Panel Analysis, Applied Health Economics and Health Policy
Impact of complete lockdown on total infection and death rates: A hierarchical cluster analysis, National Center for Biotechnology Information
Impact of lockdown on Covid-19 case fatality rate and viral mutations spread in 7 countries in Europe and North America, National Center for Biotechnology Information
How we should respond to the Coronavirus SARS-CoV-2 outbreak: A German perspective, National Center for Biotechnology Information
Impact of lockdown on COVID-19 prevalence and mortality during 2020 pandemic: observational analysis of 27 countries, National Center for Biotechnology Information
Are Lockdown Measures Effective Against COVID-19?, National Center for Biotechnology Information
Coronavirus Disease 2019 Epidemic Doubling Time in the United States Before and During Stay-at-Home Restrictions, The Journal of Infectious Diseases
52. Japan’s Covid Nightmare, Ramesh Thakur, Brownstone Institute
And, Why Does No One Ever Talk About Sweden Anymore?, Unmasked, Ian Miller
54. Coronavirus: What's going wrong in Sweden's care homes?, BBC News
See also: Sweden's nursing home COVID failures haunt relatives left behind, Reuters
55. Excess Mortality in Sweden and Denmark the Same During Pandemic Despite Sweden Refusing Lockdown, The Daily Sceptic
56. Excess mortality during the Coronavirus pandemic (COVID-19), Our World in Data
57. Excess Mortality in Sweden and Denmark the Same During Pandemic Despite Sweden Refusing Lockdown, The Daily Sceptic
58. As if Expendable: The UK Government’s Failure to Protect Older People in Care Homes During the COVID-19 Pandemic, Amnesty International UK
59. Timing of State and Territorial COVID-19 Stay-at-Home Orders and Changes in Population Movement — United States, March 1–May 31, 2020, Centers for Disease Control
And, States that did not issue stay-at-home orders in response to the coronavirus (COVID-19) pandemic, 2020, Ballotpedia
60. A Closer Look at the States that Stayed Open, American Institute for Economic Research
61. A Final Report Card on the States’ Response to COVID-19, National Bureau Of Economic Research
See also, New Covid Study Shows Lockdown-Heavy States Had Some of the Worst Health Results, Mises Institute
It is also the case that States with the worst pre-COVID health scores are the States where antibiotic use is highest, and would have therefore been impacted the most from the fall away in prescriptions.
See, All-cause mortality during COVID-19 - No plague and a likely signature of mass homicide by government response, Denis Rancourt
And, Nature of the COVID-era public health disaster in the USA, from all-cause mortality and socio-geo-economic and climatic data, Denis Rancourt
And, Lockdowns Did Not Save Lives, Brownstone Institute, Dr. John Johnson and Dr. Denis Rancourt
62. Japan’s Covid Nightmare, Ramesh Thakur, Brownstone Institute
63. Explanations for this have been debated in The Daily Sceptic:
Do Lockdowns Work?, Will Jones
And, Lockdown ‘Worked’ in Some Places, But That Doesn’t Mean It Was Justified, Dr. Noah Carl
65. Op-Ed: Do 'Lockdowns' Work?— And, if so, how much?, Vinay Prasad
See also Dr. Prasad’s presentation
66. UN Report: Global hunger numbers rose to as many as 828 million in 2021, World Health Organization
Six-fold increase in people suffering famine-like conditions since pandemic began, Oxfam report
World hunger, malnutrition soared last year mostly due to COVID-19 - U.N. agencies, Reuters
67. Lockdown’s cancer bomb may soon be worse than Covid itself, The Telegraph, Professor Karol Sikora
68. As if Expendable: The UK Government’s Failure to Protect Older People in Care Homes During the COVID-19 Pandemic, Amnesty International UK
69. Lockdowns and the Loss of Love and Family, Brownstone Institute, Mark Oshinskie
70. What’s behind the mystery of thousands of excess deaths this summer?, The Guardian
The U.K. think tank, the Centre for Social Justice has now released a report assessing the costs of lockdown on British society: Two Nations: The State Of Poverty in the UK
See a lockdown specific summary: The Costs of Lockdown - A Report from the Centre for Social Justice
71. The Annals of Tacitus, quoted from COVID-19 (excess) mortalities: viral cause impossible—drugs with key role in about 200,000 extra deaths in Europe and the US alone, By Torsten Engelbrecht, co-authored by Claus Köhnlein, MD, Real News Australia
Four. Vaccination
1. ‘Who’s going to take the shot?’, twitchy
2. Remarks by President Biden on Fighting the COVID-19 Pandemic, The White House
3. Noam Chomsky says the unvaccinated should just remove themselves from society, National Post
4. COVID-19: Democratic Voters Support Harsh Measures Against Unvaccinated, Rasmussen Reports
5. Tony Blair calls for new pass to allow vaccinated people more freedoms, The Guardian
6. ‘Tens of thousands’ of NHS and care home staff could quit over Covid jabs, The Guardian
7. Care workers sacked for refusing to get Covid-19 vaccine can get their job back as Government scraps jabs law, The i News
And, Mandatory Covid-19 vaccination dropped for nurses in England, Nursing Times
And, Judge tosses NYC COVID vaccine mandate, orders fired city workers’ back pay, New York Post
8. Factory Girl’s Resistance, American Tobacco Company’s Employees’ Fight Against Compulsory Vaccination, New York Times, April 12, 1901.
Quoted from Dissolving Illusions, Disease, Vaccines, and the Forgotten History, by Suzanne Humphries MD and Roman Bystrianyk
Other examples include:
‘England, August 1869: In August [1869] Mrs. Anne Sipple was committed for seven days’ hard labor—an illegal sentence—and confined in a stone cell with an infant of eighteen months, the child deprived of shoes and socks, and a diet of bread and water only for both.’
‘Atlanta, Georgia, December 17, 1897: Miss L. Miller a modiste [one that produces, designs, or deals in women’s fashions] of 91 Crew Street, was fined $25.75 [esti-mated value of $680 in 2009 dollars] by Recorder Calhoun to-day for refusing to be vaccinated. She was unable to pay the amount, and was ordered to serve twenty-five days in the city prison. After having been in prison for three hours Miss Miller said she would allow her family physician to vaccinate her. She was subsequently vaccinated and released.’
‘Boston, Massachusetts, January 26, 1902: In order to stamp out smallpox, which is semi-epidemic here, the Board of Health started compulsory vaccination to-day. The work was begun in East Boston, where 125 surgeons, each accompanied by a policeman, made a house-to-house canvass, vaccinating all who had not been recently inoculated. Those who refused to allow the operating will be hauled into court.’
‘There was some excitement in this city and Deadwood last night when several hundred miners were forcibly vaccinated. So many cases of smallpox has occurred in the two cities that an order was issued compelling vaccination. The miners refused. Last night the Sheriff, five deputies, and four policemen accompanied the City Physician and four assistants in a round-up of the saloons, theatres, and gambling dens . . . Several fights occurred, but the miners were overawed . . . At first the miners were disposed to be ugly, but finally turned it off in merriment but for some time last night it appeared a riot would ensue.’
‘Montreal, Canada, September 28, 1885: The by-law passed by the Provincial Board of Health making vaccination compulsory having appeared in the Official Gazette increased the excitement among the French Canadians to such an extent that a riot broke out in the east end this morning, and before the crowd dispersed they smashed many of the windows of the East End Health Office . . . some 50 police had meantime arrived and drove the mob down the street, but they immediately gathered on the Champ de Mars in the rear, where a lively hand-to-hand conflict took place, but the rioters, when dispersed at one place, immediately met at another and renewed the stone throwing, and several of the police were wounded . . . the mob returned to the house of Dr. Laporte, pub-lic vaccinator, and set fire to it . . . the rioters proceeded once more to the East End Health Office, and easily overpowered the five policemen who were on guard. The whole front of the office was torn out and the smallpox placards and sulphur for disinfecting houses were piled up in the middle of the street and set fire to . . . The police then charged the crowd and drove them out to the city limits. The clubs were plied with vigor and many of the rioters were badly cut about the head.’
9. Data from Public Health England, quoted from, Why Dr Suzanne Humphries, an anti-vaccine activist, is lying to you about measles, Isabella B.
Dr. Humphries response can be read at, Response to “Isabella B’s” “Why Dr Suzanne Humphries, an anti-vaccine activist, is lying to you about measles” by Suzanne Humphries, MD and Roman Bystrianyk
10. Graph based on Office of National Statistics data, quoted from,Quoted from Dissolving Illusions, Disease, Vaccines, and the Forgotten History, by Suzanne Humphries MD and Roman Bystrianyk
11. Focused Protection, the Great barrington Declaration
12. Pursuing COVID-19 herd immunity is unethical, WHO chief says, Leader-Telegram
13. Dr. Anthony Fauci said lockdowns are a method for coercing people to comply with COVID-19 vaccinations, PolitiFact
14. What you need to know about the COVID-19 vaccine, Bill Gates
15. Here’s why the WHO says a coronavirus vaccine is 18 months away, The Conversation
16. See Wikipedia article on COVID-19 vaccines
17. This section draws on The Anatomy of Big Pharma’s Political Reach, Brownstone Institute, Rebecca Strong
18. Timeline: The Rise and Fall of Vioxx, National Public Radio
19. Testimony of David J. Graham, MD, MPH, United States Senate
20. Did the FDA ignite the opioid epidemic?, CBS News
‘Equally suspicious but legal, the large number of key FDA regulators who went through the revolving door to jobs with drug manufacturers. The two medical officers, who originally approved Oxycontin, Curtis Wright and Douglas Kramer, went to work for the opioid maker, Purdue Pharma, not long after leaving the FDA.’
21. Lucrative Drug, Danger Signals and the F.D.A., New York Times
22. Pfizer drug breach ends in biggest US crime fine, The Guardian
23. Pfizer whistleblower's ordeal reaps big rewards, Reuters
24. Pfizer Bribed Nigerian Officials in Fatal Drug Trial, Ex-Employee Claims, CBS News
25. Pharmaceutical Giant AstraZeneca to Pay $520 Million for Off-label Drug Marketing, United States Department of Justice
26. AG Paxton Recovers $110 Million for Texas in Medicaid Fraud Settlements, Texas Attorney General
27. Ex-sales manager-turned-whistleblower takes AstraZeneca to court in retaliation trial set for next week, Fierce Pharma
28. Covid: FDA approves Pfizer vaccine for emergency use in US, BBC
Covid: US approves Moderna as second vaccine, BBC
Covid vaccine: Single-dose Johnson & Johnson jab is 66% effective, BBC
Covid-19: Oxford-AstraZeneca vaccine approved for use in UK, BBC
29. The AstraZeneca vaccine is 100% effective....., Professor Norman Fenton
30. The Vaccine Was “95% Effective” How?, Brownstone Institute, Robert Blumen
And, COVID-19 vaccine efficacy and effectiveness—the elephant (not) in the room, The Lancet
31. “Open a Public Inquiry into Covid-19 Vaccine Safety”: Response to the UK Government’s Response, Where are the Numbers?, Axel McFarlane and Mike Baker
‘311 (1.4%) vaccine recipients vs 61 (0.3%) placebo recipients were excluded from the trial for “protocol deviations” (page 30). There is an infinitesimal probability of this happening by chance, but no explanation is given. The most likely cause, an adverse reaction causing the participant to withdraw from the trial, would have shown that the vaccine had a highly-negative safety profile.’
32. Covid-19: Researcher blows the whistle on data integrity issues in Pfizer’s vaccine trial, The British Medical Journal
33. Serious adverse events of special interest following mRNA COVID-19 vaccination in randomized trials in adults, Vaccine
34. Covid: Who is not vaccinated in the US and what's the risk?, BBC
Latest CDC Data: Unvaccinated Adults 97 Times More Likely to Die from COVID-19 Than Boosted Adults, Factcheck.org via the Washington Informer
35. Covid deaths rare among fully vaccinated - ONS, BBC
36. Global impact of the first year of COVID-19 vaccination: a mathematical modelling study, The Lancet
See also, COVID-19 vaccines saved nearly 20 million lives in a year, study says, CBS News
37. Graph from Factcheck.org constructed using CDC data
38. COVID-19 vaccines have enhanced reporting requirements for vaccine safety database, so death reports cannot be simply compared to other vaccines, Health Feedback
39. Ibid
Articles on Professor Fenton’s team’s work are published at Where are the Numbers?
41. This example is taken from Professor Fenton’s presentation, How Flawed Statistics Have Manipulated The Covid Narrative
42. What the ONS Mortality Covid-19 Surveillance Data can tell us about Vaccine Safety and Efficacy, report to the UK Statistics Regulator
43. ONS Deaths by Vaccination Status statistics, UK Statistics Regulator
44. A critique of the BBC2 documentary “Unvaccinated”, Professor Norman Fenton
See also, BBC response to my complaint about "Unvaccinated", Professor Norman Fenton
And, Exploring attitudes towards Covid-19 vaccinations, Walnut Unlimited
‘ICM Unlimited interviewed a sample of 2,570 UK residents, including 1,894 vaccinated residents (who had received at least one dose of the Covid-19 vaccination), and 664 unvaccinated residents (who had not received any Covid-19 vaccinations, either through choice or medical exemption). The data were weighted to be representative of the UK population in terms of demographics and vaccination take-up.’
Professor Fenton comments that:
‘Based on that survey, there is essentially zero probability that the true population unvaccinated percentage is less than 20%. In fact, there is a 99.973% probability the proportion of unvaccinated is at least 23%.’
45. ONS Deaths by Vaccination Status statistics, UK Statistics Regulator
46. The latest ONS data on deaths by covid vaccination status, Professor Norman Fenton
And, Claims the unvaccinated were at higher risk of hospitalisation and death were based on deliberately murky record keeping, Professor Martin Neil and Professor Norman Fenton
47. What the ONS Mortality Covid-19 Surveillance Data can tell us about Vaccine Safety and Efficacy, report to the UK Statistics Regulator, Fenton, et al
48. Dr. Susan Oliver presents this explanation in her presentation Lies, damn lies, and Fenton/Campbell misrepresentation of ONS statistics. Dr. Oliver presents two papers in support of the long COVID explanation:
Impact of Vaccination on Major Adverse Cardiovascular Events in Patients With COVID-19 Infection, Journal of the American College of Cardiology
And, Long-term cardiovascular outcomes of COVID-19, Nature
The latter of these has been critiqued by Dr. Vinay Prasad in his article, Long term cardiovascular complications of COVID:
‘The authors do not use a sero-prevalance denominator, so they are only showing outcomes from people sick enough to seek medical care (either for covid or other reason) and then get tested for COVID. Moreover, the study cannot separate the effect of covid from the effect of getting ensnared by the medical system. There is an old saying in medicine, “show me a healthy person, and I will show you someone who has not had enough tests.” The more you test the people who come to the hospital, the more diagnoses you will find. The control patients did not get the full force of American testing exceptionalism.’
For more on long COVID studies see, Heart attacks and strokes after a COVID diagnosis, Dr. Vinay Prasad
‘The paper compares people who meet a post covid condition definition, using a CDC definition to uninfected controls. Many people who had COVID do not meet this definition and are fine. It compares a tiny set of people who had covid— those with a post covid condition— to the uninfected.’
And, A Short History of Long Covid, Brownstone Institute, Professor Steve Templeton
49. What the ONS Mortality Covid-19 Surveillance Data can tell us about Vaccine Safety and Efficacy, report to the UK Statistics Regulator, Fenton, et al
50. Ibid
51. Official mortality data for England suggest systematic miscategorisation of vaccine status and uncertain effectiveness of Covid-19 vaccination, Professor Martin Neil et al.
52. Norman Fenton and John Campbell discuss latest ONS deaths by vaccination status data
53. ONS Deaths by Vaccination Status statistics, UK Statistics Regulator
‘In your paper you also state that the number of deaths reported within the first 21 days of receiving the first dose of the Covid-19 vaccination is below that which could be expected in the general population, and that this difference is evidence of systematic undercounting of deaths by ONS. Our view of this question starts with the consideration that the population included is not representative of the general population, and it is therefore likely that any pattern you observe is attributable to the ‘healthy vaccinee’ effect. This happens when people who are ill (either due to COVID-19 or another relevant illness) are likely to delay vaccination. The result of this effect is a lower-than-average mortality rate within the first 21 days of receiving a vaccination. This effect is described by ONS in their Deaths by Vaccination Status publication.
‘Turning to the underlying data recording, we do not consider that there is evidence to indicate that ONS has systematically undercounted deaths within the first two weeks of receiving the COVID-19 vaccination. ONS have confirmed with us that they do receive data in these instances, and that the individual would fall into the ‘vaccinated’ category. We have asked that this be made clear in future iterations of this publication.
‘ONS has previously published information on the number of people who died after receiving the COVID-19 vaccination (up to January 2022, there were 24 deaths registered in the UK with ICD-10 code U12, COVID-19 vaccines causing adverse effects, on the death certificate). When we met with ONS, it confirmed that it is working on a publication that focuses on deaths after the COVID-19 vaccination, which will be published this year.’
54. COVID-19 vaccine effectiveness estimated using Census 2021 variables, England: 31 March 2021 to 20 March 2022, Office of National Statistics
55. Swedish Public Health Agency reporting has distorted mortality rates for the unvaccinated and the vaccinated, Läkaruppropet
56. SARS-CoV-2 Infections and Hospitalizations Among Persons Aged ≥16 Years, by Vaccination Status, Centers for Disease Control
See also, Covid-19: Definitions matter - and these are REAL, Professor Norman Fenton
57. Official mortality data for England suggest systematic miscategorisation of vaccine status and uncertain effectiveness of Covid-19 vaccination, Professor Martin Neil et al.
‘In previous years, each of the 60-69, 70-79 and 80+ groups have mortality peaks at the same time during the year (including 2020 when all suffered the April Covid peak at the same time). Yet in 2021 each age group has non-Covid mortality peaks for the unvaccinated, at a different time, namely a time shortly after the vaccination rollout programmes for those cohorts reach a peak, which for 60-69, 70- 79 and 80+ age groups was week 7, week 5, and week 1 respectively.’
58. Claims the unvaccinated were at higher risk of hospitalisation and death were based on deliberately murky record keeping, Professor Norman Fenton
See also, Update on the flawed hospital data, Professor Norman Fenton
59. Fact check: "The covid vaccine is safe for pregnant women", Professor Norman Fenton
And, Why are UKHSA obfuscating data on stillbirths by vaccine status: just another statistical illusion?, Professor Norman Fenton
60. How the CDC looked for safety signals in the covid vaccines, Professor Norman Fenton
61. Unequivocal Safety Signals for Heart, Blood and Reproduction Found in Yellow Card Vaccine Data, Says Top Scientist – “Withdraw Them Immediately”, The Daily Sceptic, Dr. Richard Ennos
Five. Viral Origins
1. 99 Red balloons, Nena
2. Coronavirus: China’s first confirmed Covid-19 case traced back to November 17, South China Morning Post
3. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China, The Lancet
4. The First 50 days of COVID-19: A Detailed Chronological Timeline and Extensive Review of Literature Documenting the Pandemic, Elsevier
5. Wuhan Municipal Health and Health Commission's briefing on the current situation of pneumonia in our city
And, National Health and Medical Commission expert team found pneumonia of unknown cause in Wuhan, CCTV
6. Press Release, Hong Kong Government
And, CDC implements extra inspection measures for Wuhan flights, Taiwan Today
7. Exclusive: U.S. axed CDC expert job in China months before virus outbreak, Reuters
8. The Lost Month: How a Failure to Test Blinded the U.S. to COVID-19, New York Times
9. China Pneumonia Outbreak Spurs WHO Action as Mystery Lingers, Bloomberg
10. Analysis: Did Trump offer experts to China to help with the coronavirus?, Washington Post
11. China pneumonia outbreak: Mystery virus probed in Wuhan, BBC
12. Notes from the Field: An Outbreak of NCIP (2019-nCoV) Infection in China — Wuhan, Hubei Province, 2019−2020, China CDC Weekly
13. China Grapples With Mystery Pneumonia-Like Illness, New York Times
14. Highlights: China's Xi recounts early role in coronavirus battle, Reuters
15. How bad was flu season this year in New York? Spoiler alert: Record breaking, lohud
16. China hunts cause of mysterious pneumonia outbreak in Wuhan, Axios
18. Where’s the Emergency?, Viroliegy, Mike Stone
19. Similarities and Differences between Flu and COVID-19, US Centers for Disease Control
20. Notes from the Field: An Outbreak of NCIP (2019-nCoV) Infection in China — Wuhan, Hubei Province, 2019−2020, China CDC Weekly
21. Researchers develop first diagnostic test for novel coronavirus in China, German Center for Infection Research
22. Corman-Drosten Review Report Curated By An International Consortium Of Scientists In Life Sciences (Icsls)
See also, Dr. Kevin Corbett, a co-author of the retraction request, being interviewed on Oracle Films
23. Ibid
24. “Viral” Load of Crap, Viroliegy, Mike Stone
25. For criticism of PCR testing, we would recommend starting with the short presentation: The Truth About PCR Tests, by Dr. Sam Bailey, Dr. Bailey has an extensive series of presentations on PCR
Also recommended are:
PCR tests at Viroliegy, by virus researcher Mike Stone
Corona Hysteria, at the website of Dr. Kevin Corbett
The Viral Delusion, documentary series produced by Michael Wallach
Virus Mania: How the Medical Industry Continually Invents Epidemics, by Torsten Engelbrecht, Claus Köhnlein, MD, Dr. Samantha Bailey, MD and Dr. Stefano Scoglio
26. This example is taken from Professor Norman Fenton’s presentation, How Flawed Statistics Have Manipulated The Covid Narrative
27. Faith in Quick Test Leads to Epidemic That Wasn’t, The New York Times
28. The Self-Fulfilling Prophecy: What It Is and How It’s Used in Fiction, TCK Publishing
Conclusion
1. Triggernometry Interview, with Dr. John Campbell
2. The Four Pests Campaign, Wikipedia
3. The Moth in the Iron Lung, A Biography Of Polio, Forrest Maready
See also, We tried to get rid of mosquitoes once. It didn’t work out so well, CNN
4. Did New Zealand PM Jacinda Ardern Once Say, 'Unless You Hear It from Us, It Is Not the Truth'?, Snopes
5. Fauci: Attacks on me are really also ‘attacks on science’, The Hill
6. To Take On the Coronavirus, Go Medieval on It, The New York Times