Subsidies to increase utilization are used in all sorts of fields and I have read more than my fair share of CCT papers. However, until last week, I had not come across a scheme that paid people to purchase their urine. Given that I am traveling and the fact that I am missing Halloween, I thought I’d share (I hope it’s not TMI)…
Here is the abstract of an article by Tilley and Günther (2016), published in Sustainability:
“In the developing world, having access to a toilet does not necessarily imply use: infrequent or non-use limits the desired health outcomes of improved sanitation. We examine the sanitation situation in a rural part of South Africa where recipients of novel, waterless “urine-diverting dry toilets” are not regularly using them. In order to determine if small, conditional cash transfers (CCT) could motivate families to use their toilets more, we paid for urine via different incentive-based interventions: two were based on volumetric pricing and the third was a flat-rate payment (irrespective of volume). A flat-rate payment (approx. €1) resulted in the highest rates of regular (weekly) participation at 59%. The low volumetric payment (approx. €0.05/L) led to regular participation rates of only 12% and no increase in toilet use. The high volumetric payment (approx. €0.1/L) resulted in lower rates of regular participation (35%), but increased the average urine production per household per day by 74%. As a first example of conditional cash transfers being used in the sanitation sector, we show that they are an accepted and effective tool for increasing toilet use, while putting small cash payments in the hands of poor, largely unemployed populations in rural South Africa.”
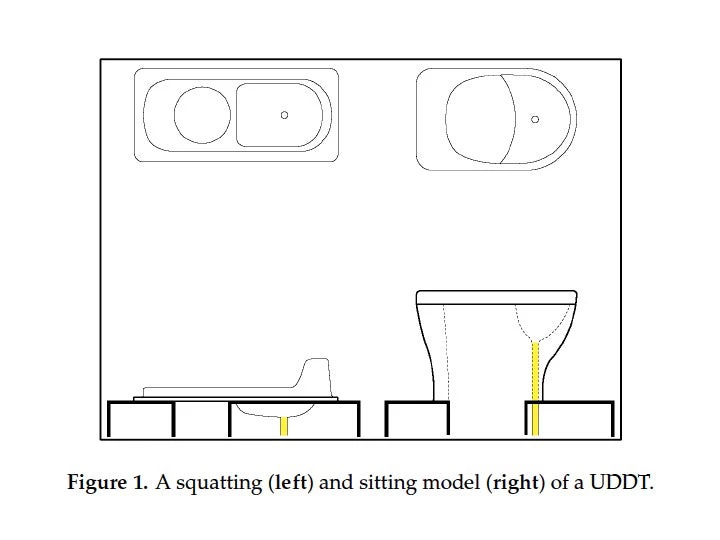
No, this is not from the Onion or something I made up for a goofball Halloween post: it is a real experiment two researchers ran in rural areas near Durban, KwaZulu-Natal. Urine-diverting dry toilets (UDDTs), which were installed by the local water and sanitation unit, look like this:
Amazingly, apparently the good people of eThekwini did not warm up to these beauties. The authors tell us why:
“With the urine separated, the faeces fall into and are collected in one of two dehydration chambers. The separation means that smells are reduced (since bacterial growth is limited in the absence of moisture) and emptying the chambers is much easier compared to a pit latrine. However, the separation at the user interface is not perfect and the user must “aim” in order to get the urine in the front to keep the faeces chambers dry and prevent clogging in the urine pipe; the seat is especially difficult for children to use. Though households did not have to pay for the installation, and do not need to pay for water (to make them work), evidence suggests that acceptance and use rates are low.”
No shit…
Of course, the main goal in sanitation programs like these is to prevent open defecation (rather than simply urination). The authors explain why they focused on urine:
“The overarching goal of this research was to determine the impact of CCTs on toilet use and although toilets are used for both urination and defecation, we only incentivized and measured the quantity of urine. We proceeded in this way for several reasons: First, faeces are difficult and messy to measure, especially compared to the simple toilet retrofit that allowed us to measure urine without any direct impact on the user (see below). Second, urination is about 3–5 times more frequent than defecation meaning that variation would be easier to measure. By incentivizing urine collection, we were hoping to habituate the more repetitive behaviour, which would in turn have a more long-lasting effect. Third, we assumed that some users (primarily men) would have little incentive to use a fixed toilet to urinate (given the vast, rural area), but would be more inclined to defecate in the privacy of the built structure; the CCT would target this behaviour gap directly. So although urine is not a perfect proxy, it was a practical and reasonable estimator of the willingness of participants to use a toilet.”
OK.
So, in treatment areas, the researchers cut the pipes that allow the urine to infiltrate directly into the soil and installed 20L jerry cans to collect the urine that beneficiaries could sell to them:
I was going to discuss some of the methods and findings, but then I realized that (a) communities were not assigned to treatment randomly, (b) there were only three control and two treatment communities, and perhaps most worryingly (c) treatment and control communities looked different than each other in all aspects (see Table 1). As there were other things about the intervention rollout (such as the interventions following each other over time in the same community) that were hard to understand, I am choosing not to.
If the paper doesn’t tell us much with respect to conditional cash transfers – other than confirming the economists’ mantra that “everything has a price” – it does remind us about the difficulties practitioners and local governments in this sector face. Technological change that makes products convenient to use for the target population is hugely important in all sorts of fields (think family planning, for example), and toilets seem to belong squarely in that category. I see a Gates Challenge Grant in the horizon…
(Coincidentally, last month at the Behavioral Economics and Global Health Conference at UC Berkeley, Reshmaan Hussam presented her work on habit formation and the theory of rational addiction (Becker and Murphy 1988), which she applies to hand washing with soap (PDF, video). Brilliant work – I highly recommend it. In fact the whole conference had a lot of nice papers and was really enjoyable.)
Bottom line (no pun intended): Paying 1 Rand per liter of urine increased urine sales in from the jerry cans by 74% over the comparison group, albeit with lower participation rates. It’s not clear whether the treatment subsidized additional liquid consumption (water, soft drinks, coffee/tea, beer) or actually switched people from relieving themselves in the bush to aiming into the bowl...

Join the Conversation