There's Probably Way More Zika in the United States Than Has Been Counted
New computer modeling suggests the virus has been underestimated by tens of thousands of cases.

Try as they might, public-health officials can’t really track the Zika virus in real time. There is inevitably a lag between how a disease spreads and when the public finds out about it.
Even in Miami, where new updates are being issued every weekday, there’s only so much officials know about how quickly and widely Zika is traveling through the population.
Then there are the unknowns that are harder to pin down: How many cases of Zika are going uncounted? It turns out, that number may be enormous.
Researchers at Northeastern University say federal-health officials are likely vastly undercounting Zika in the United States. In a paper that’s still under review for journal publication, they describe computer modeling that suggests there were nearly 30,000 cases of travel-related Zika in the country in mid-June, about 25 times more cases than the 1,200 or so reported by the CDC at the time.
Researchers found the undercounting occurred in at least nine states: Florida, California, Texas, Georgia, Illinois, North Carolina, Ohio, Indiana, and Oregon.
“CDC is doing a great job, but it is really hard to detect cases,” said Alessandro Vespignani, one of the authors of the paper. The federal agency is faced with an exceedingly difficult task, in part because it is cobbling together data from various monitoring systems in different states and jurisdictions. The nature of the virus presents additional challenges, making it more complicated to track than other epidemics. “You have to ingest much more data and deal with another level of complexity as well as other sources of uncertainties,” Vespignani said.
Because Zika is transmitted by mosquitoes (as well as spread between humans), researchers trying to model or predict its path have to take into consideration the presence of certain mosquito species, mosquito populations in different areas, that population’s variability with weather conditions, and so on. (Northeastern’s computer model does not take sexual transmission of Zika into consideration, even though it’s one of the ways the virus is transmitted.)
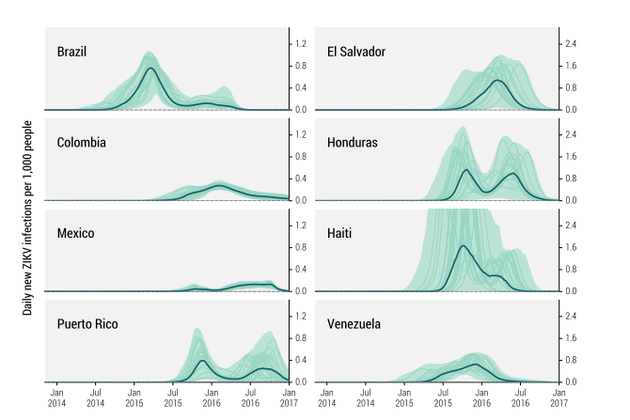
Vespignani and his colleagues also used their model to predict how Zika will continue to move through the Americas through the end of 2016, based on how it has spread globally since 2013. (They also took into account the rate of transmission of Dengue in various regions, since that virus has much in common with Zika.)
The modeling suggests that while the Zika epidemic has already peaked in Brazil, the number of cases is still growing rapidly in Puerto Rico, and will continue to climb well into the fall. And while the researchers say their findings should be interpreted cautiously, given the complexity of the modeling, they believe their projections offer important indications of “the magnitude and timing” of the epidemic as it progresses.
There are other computer-modeled predictions that could be useful—the estimated number of cases of Zika-related Microcephaly, a brain defect in which newborns have abnormally small heads, for example. But modeling such outcomes, especially when so much remains unknown about Zika, is difficult if not impossible without more robust clinical data. “Models can be only as good as the data they ingest,” Vespignani said.
For the CDC, good data may be the central challenge in tracking Zika. Because the agency only counts confirmed cases of the disease, and because people who catch Zika are usually asymptomatic, there are almost certainly a significant number of people who have had the virus without knowing it.
“Like the [Northeastern University] team, when we work on estimating components of the epidemic, we try to understand the dynamics of infection relative to the available information, always under the assumption that what we ‘see’ through surveillance is only the tip of the iceberg,” said Michael Johansson, a biologist in the CDC Division of Vector-Borne Diseases, in a statement provided to The Atlantic by a spokesman. “Many infections are asymptomatic, some are mild with symptoms that do not cause people to seek care, some cases are mistaken as other diseases, and then we get to the diagnostics which are also challenging.”
“All of those components contribute to many fewer cases being reported than the number of infections that actually occurs,” Johansson said.
What does all of this mean for people who just want to protect themselves from the virus? Zika should be taken as the serious threat to public health that officials have said it is. Though many cases of Zika are mild, scientists are just beginning to understand how devastating it can be—including among children and adults sickened by the disease, not just fetuses. In Utah, one man died from the virus. (And officials still don’t understand how a family member who cared for him contracted Zika.)
The CDC has clear guidelines on how people—particularly pregnant women—can protect themselves from the virus. Until scientists learn more about how Zika spreads and how it might be stopped, it’s important to understand it could be much more widespread than it appears.