
Abstract
Background
The vast majority of research on HIV-related stigma has been cross sectional, and few studies have examined whether experiencing stigma is associated with sexual risk behaviors.
Purpose
The purpose of this study is to examine the prospective relationships between experiencing HIV-related stigma and symptoms of anxiety and depression, as well as sexual transmission risk behavior.
Methods
The sample included HIV-infected men who have sex with men (n = 314) who participated in a secondary HIV-prevention study at their primary care site. Participants were assessed at baseline, and then completed follow-up assessments at 3, 6, 9, and 12 months.
Results
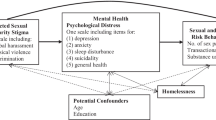
Experiencing HIV-related stigma was prospectively associated with symptoms of depression (β = 0.16, p < .001), panic (β = 0.11, p = .01), and generalized anxiety (β = 0.05, p = .05). In addition, perceiving HIV-related stigma was prospectively associated with transmission risk behaviors, including unprotected receptive or insertive anal intercourse with HIV-seronegative or status unknown partners (β = 0.06, p = .047).
Conclusions
Experiencing HIV-related stigma may increase risk for sexual transmission risk behavior and mental health problems.
Similar content being viewed by others


Introduction
Stigma associated with HIV is a common experience for many HIV-infected individuals, both domestically [1] and internationally [2]. Not only does stigma create structural difficulties for those living with HIV, such as discrimination by health care professionals [3], but it also leads to poor health outcomes. Indeed, a recent meta-analysis of 24 peer-reviewed studies that have been conducted in North America since January 2000 indicated that perceived stigma related to HIV is associated with several adverse outcomes among HIV-infected individuals, including depression and biomarkers of disease progression, such as CD4 count [4].
Despite the fact that men who have sex with men (MSM) account for over half of all prevalent HIV cases in the USA [5], researchers have only recently begun to examine the prevalence and correlates of HIV-related stigma among this group. Existing studies of youth [6] and adult MSM [7, 8] have demonstrated significant associations with mental health problems and social isolation. These studies have provided important insights but have relied on cross-sectional designs. In fact, all but one of the 24 studies included in the recently published meta-analysis of HIV-related stigma (which included two studies on MSM) were cross sectional [4]. Prospective data are therefore needed to establish stronger causal inferences.
In addition, whereas numerous studies have examined associations between HIV-related stigma and mental health outcomes in MSM, there has been limited investigation of whether HIV-related stigma is associated with HIV transmission risk behaviors. Evidence from cross-sectional studies of MSM has been mixed. One study [7] failed to document associations between HIV-related stigma and sexual risk behaviors (i.e., unprotected anal intercourse with partners of negative or unknown serostatus), whereas another study found only indirect associations through sensation seeking [9]. If HIV-related stigma were shown to be prospectively predictive of increased sexual risk behaviors, this would have important implications for public health interventions.
The current study had two primary aims: (a) to evaluate perceptions of HIV-related stigma as a prospective predictor of mental health problems, including symptoms of depression and anxiety; and (b) extend prior work by examining prospective relations between perceived HIV-related stigma and HIV transmission risk behaviors. A secondary aim was to examine whether mental health symptoms mediated the association between perceived stigma and HIV risk behaviors, given previous cross-sectional findings showing higher rates of depression among HIV + MSM who engaged in sexual risk behaviors [10]. We used longitudinal data from a diverse sample of HIV-infected MSM (N = 314) to test these aims.
Methods
Participants
The sample is comprised of HIV-infected MSM who participated in either one of two concurrently run secondary HIV-prevention studies. Both interventions utilized a four-session cognitive behavioral curriculum, one integrated into prevention case management delivered by social workers and the other intervention delivered by peer counselors, both with the primary outcomes to reduce HIV sexual transmission risk. The sample is described in detail elsewhere [11, 12]. Inclusion criteria included: (a) HIV positive, (b) 18 years of age or older, (c) self-identified as a man who has sex with men, (d) receiving primary HIV care at Fenway Community Health [13], and (e) completion of baseline and at least one other follow-up assessment (a requirement of the hierarchical linear modeling (HLM) analyses used).
Procedures
Data were collected via surveys administered through the Audio Computer-Assisted Self-Interview system. The survey lasted for approximately one hour. Respondents completed the surveys at baseline, and then again at 3, 6, 9, and 12 months.
Measures
Perceived HIV-Related Stigma
Two items were used to assess perceived HIV-related stigma: [1] “Most people are afraid to be around people with HIV”; and [2] “I feel ashamed that I have HIV.” Responses ranged from “strongly disagree” [1] to “strongly agree” [7]. Because these two items were significantly correlated (r=.28, p<.001), they were summed to create a total stigma score (ranging from 2 to 14). These items were taken from a series of questions designed to assess attitudes and beliefs about a broad range of issues related to living with HIV for use in a multi-site prevention study with HIV-infected individuals, funded through the Health Resources and Service Administration [14].
HIV Transmission Risk Behaviors
Transmission risk behavior was defined as the number of instances of unprotected insertive or receptive anal intercourse with HIV-uninfected or unknown status partners within the past 3 months. These items were adapted from prior HIV Transmission Risk Behavior research trials with MSM [15] where participants were asked about each type of sexual act by partner status (positive, negative, and unknown). All self-report data were collected via audio computer-assisted self-interview to increase the chances of self-reporting sensitive HIV risk behaviors.
Depression
Depression symptoms were measured by the 9-item depression severity scale of the Patient Health Questionnaire, which is used to help primary care providers identify and diagnose mental health disorders [16]. The Patient Health Questionnaire Depression Severity Scale has demonstrated high internal consistency reliability, test-retest reliability, and strong construct validity [17]. The scale demonstrated excellent internal reliability in the current sample (Cronbach’s α = .92).
Anxiety
Anxiety symptoms were assessed with 14 items from the Patient Health Questionnaire [16]. Specifically, panic disorder was assessed through the Panic Disorder Severity Scale of the Patient Health Questionnaire (diagnostic accuracy of 98%), and generalized anxiety was measured through its sub-scale of the Patient Health Questionnaire (diagnostic accuracy of 91% for any anxiety disorder) [16]. The scale demonstrated good internal reliability in the current sample (panic: Cronbach’s α = .77; generalized anxiety: Cronbach’s α = .78).
Statistical Analyses
HLM 6.0 [18] was used in order to examine HIV transmission risk behavior and symptoms of depression and anxiety over time, as well as how changes in perceived HIV-related stigma influenced these outcomes. In a longitudinal HLM framework, interviews are nested within individuals. In such a model, estimates of effects are estimated for each individual from data that he contributed over the course of the study. Individual intercepts and slopes (changes across time) are estimated from available data. A distinct advantage of the HLM approach is that it allows for modeling within-individual variation over time. In addition, it handles missing and unbalanced data better than other statistical procedures typically used with repeated-measures data.
In HLM, level 1 is the repeated-measures (intra-individuals) level, and level 2 is the between-subjects (inter-individuals) level. We chose to model all of our data points as level 1 variables because we wanted to capture the variability in perceived HIV-related stigma experiences that occurred within individuals across time (i.e., the time-varying nature of this predictor). We thought it was especially important to model our data in this way given that an individual’s social environment, and the concomitant cognitive, affective, and behavioral responses to this environment, involve dynamic changes over time. In addition, there were no significant associations between demographic characteristics of the sample (age, race/ethnicity, and education) and our independent or dependent variables. For this reason, there were no demographic predictors at level 2. The predictor variable (i.e., perceived stigma) was grand centered so that the value of zero represented the grand mean for the sample for that particular variable.
Within HLM, unconditional growth models were initially tested to evaluate the extent to which there is variability in intercepts and slopes across individuals in order to test the viability of adding more predictors. In unconditional growth models, time is the only predictor of the outcome of interest that is modeled. The time variable represented the number of months from the baseline assessment for each individual participant in order to indicate the varying time intervals between the assessment points. Fixed effects for the slopes were then assessed to determine the extent to which there were significant increases or decreases in HIV transmission risk behavior and depressive and anxious symptoms across time.
After testing the unconditional models, perceived HIV-related stigma was entered as a level 1 time-varying predictor of HIV transmission risk behavior and symptoms of depression and anxiety over time. We ran two models. In the first model, we tested for concurrent associations between perceived HIV-related stigma and the slopes of our outcome variables at each time point. Given that the correlation between the two stigma items was low, despite being statistically significant, we present the results for the sum of the items, as well as for the two items separately (perceived fear and shame). In the second model, we conducted time-lagged analyses, in which perceived HIV-related stigma from the immediately preceding time point was used to predict changes in HIV transmission risk behaviors and symptoms of depression and anxiety at subsequent time points. This time-lagged approach allowed for a stronger test of the predictive validity of perceived HIV-related stigma as a risk factor for adverse mental and behavioral health outcomes. Finally, we tested a mediation model examining whether depression and anxiety symptoms explained the prospective association between perceived stigma and HIV transmission risk behaviors. Sobel’s standard error approximation was used to test the significance of the intervening-variable effect [19].
Results
Descriptive Statistics
Demographic characteristics of the study sample are presented in Table 1. Across the five time points, nearly half of respondents (ranging from 43.4% to 47.6%) agreed “at least somewhat” that others are afraid to be around people with HIV. Similar rates were observed for shame surrounding one’s HIV status (responses ranging from 42.9% to 51.8%). The unconstrained growth model of perceived stigma indicated significant variability about the slope (β = −0.03, SE = 0.01, df = 313, p = .045) of stigma, providing support for modeling stigma as time-varying.
Table 2 presents the descriptive statistics for the outcome measures, including HIV transmission risk behavior and symptoms of depression and anxiety, at each of the five time points, and Table 3 presents correlations between all study variables at baseline.
Unconditional Growth Models
Prior to evaluating whether perceived HIV-related stigma predicted the outcomes of interest over time, an unconditional model with no predictor variables (other than time) was tested to assess the level of individual variability in HIV transmission risk behavior and symptoms of depression and anxiety. Variance components were tested for significance to determine whether the inclusion of parameters for random variance was needed. The variance components for the intercepts and slopes for all outcomes were significant (p < .01). Therefore, random effects were included in all subsequent models. The unconditional growth model showed that there were significant fixed effects for the slope for HIV transmission risk behavior (p < .05), reflecting that there was a significant decrease in HIV risk behavior over time. In contrast, there were no significant changes in depressive or anxiety symptoms over the course of the study.
Concurrent Associations
Perceived stigma was associated concurrently with increased risk for engaging in unprotected receptive or insertive anal intercourse with unknown or negative partners (β = 0.08, SE = 0.02, df = 309, p < .01). Because this composite variable included both receptive and insertive anal intercourse, we separated these two HIV risk behaviors in follow-up analyses. Only unprotected receptive anal intercourse was significantly associated with perceived stigma (β = 0.06, SE = 0.03, df = 250, p = .047). Analyses that separated the two stigma items demonstrated that the association between perceived stigma and unprotected receptive anal intercourse was only significant for perceived shame (β = 0.18, SE = 0.08, df = 350, p = .03).
Perceived HIV stigma was also concurrently associated with adverse mental health outcomes over the duration of the 12-month study. Specifically, greater perceptions of HIV-related stigma were associated with symptoms of depression (β = 0.16, SE = 0.03, df = 309, p < .001), panic (β = 0.11, SE = 0.04, df = 311, p = .01), and generalized anxiety (β = 0.05, SE = 0.02, df = 309, p = .01). Analyses that separated the two stigma items demonstrated that the association between perceived stigma and mental health was driven by perceived fear (depression: β = 0.11, SE = 0.05, df = 303, p = .04; generalized anxiety: β = 0.07, SE = 0.04, df = 305, p = .06).
Prospective Associations
We next used time-lagged analyses to examine whether perceived HIV-related stigma would predict the outcomes of interest at subsequent occasions. These results were similar to the concurrent analyses for the summed stigma scale. Perceived stigma predicted unprotected receptive or insertive anal intercourse with unknown or negative partners (β = 0.06, SE = 0.03, df = 223, p = .03), as well as symptoms of depression (β = 0.16, SE = 0.03, df = 222, p < .001), panic (β = 0.13, SE = 0.05, df = 223, p = .01), and generalized anxiety (β = 0.05, SE = 0.02, df = 223, p = .05). In contrast to the concurrent analyses, the individual stigma items were not differentially predictive of either the mental or behavioral health outcomes in the time-lagged analyses.
Mediation Analyses
In the mediation models, the association between perceived stigma and unprotected receptive anal intercourse remained significant after controlling for each of the three mental health symptoms (p < .05). Sobel’s tests indicated that none of the mental health symptoms served as mediators explaining the association between perceived stigma and unprotected receptive anal intercourse: depression (p = .45), generalized anxiety disorder (p = .12), and panic symptoms (p = .10).
Discussion
Previous studies of HIV-infected MSM have documented cross-sectional associations between HIV-related stigma and adverse health outcomes [6–8]. The current study extends this prior work in two ways. First, we provided prospective data documenting that perceived HIV-related stigma has deleterious consequences for mental health; perceived stigma was longitudinally associated with symptoms of depression, panic, and generalized anxiety. These results are consistent with a prior longitudinal study of HIV-infected gay caregivers of loved ones with AIDS, which also found that increases in AIDS-related stigma were associated with depressive symptoms over time [20]. However, the unique stressors of bereavement may have rendered the caregivers in this previous study more vulnerable to the effects of HIV-related stigma, thereby restricting generalizability of these results. Thus, one of the strengths of the current study is that it corroborated these earlier findings in a broader sample of HIV-infected MSM and also extended these findings by documenting additional prospective associations between perceived HIV-related stigma and symptoms of anxiety. Given that psychopathology interferes with HIV disease management, including medication adherence [21], these results provide additional evidence that HIV-related stigma may be particularly harmful for the health of HIV-infected MSM, as well as their sexual partners.
Second, our results indicated that perceptions of HIV-related stigma also lead to sexual behaviors that increase risk for HIV transmission, which may also place MSM at greater risk for sexually transmitted infections [22]. Although studies using measures of internalized homophobia [23] have documented associations with HIV risk behaviors, to our knowledge this is one of the first longitudinal studies to demonstrate that perceived HIV-related stigma in particular is predictive of sexual transmission risk behavior. Researchers have noted that MSM are at increased risk for multiple, co-occurring health problems that act synergistically to place MSM at greater risk for HIV infection [24], which has been termed “syndemics” [25]. One of the hypothesized mechanisms for syndemics in MSM is the stress associated with stigma. Results from the current study provide preliminary empirical evidence for this hypothesis and suggest that stigma may be a common vulnerability factor for psychosocial problems and health risk behaviors that are driving the HIV/AIDS epidemic among MSM.
Third, the experience of stigma has multiple affective consequences that include both vigilance for threat/danger [26] and shame [27], suggesting that these may be relevant dimensions of HIV-related stigma. Results for the concurrent (but not time-lagged) analyses revealed differential relationships between perceived fear and shame and the mental and behavioral health outcomes. In particular, perceived fear was uniquely associated with depressive and anxious symptoms, whereas perceived shame was uniquely predictive of HIV risk behaviors (unprotected receptive anal intercourse). These results are broadly consistent with studies of individuals not infected with HIV, which have shown that perceptions of fear and danger are associated with mixed depressive/anxious disorders [28]. Moreover, previous research has documented cross-sectional associations between shame and sexual risk behaviors among HIV-positive individuals with a history of childhood sexual abuse [29]. It is important to note, however, that our study used single items to assess these constructs. Future studies that utilize more comprehensive measures of fear and shame in the context of HIV are needed in order to determine whether our results are replicable.
Finally, we did not find evidence that symptoms of depression or anxiety served as a mechanism explaining the association between perceived stigma and HIV risk behaviors. Previous cross-sectional research has found that depressive symptoms (but not anxiety symptoms) are correlates of greater HIV risk behaviors among HIV + MSM [10], but other studies have failed to document such associations [30]. There were no significant changes in depression or anxiety symptoms over the course of the current study, and the scores on the mental health symptom scales were low, which restricts the variance and therefore likely limited our ability to observe prospective associations between the mental health and sexual risk behavior variables.
These results have potentially important implications for multi-level interventions. At the social/structural level, it will be important to continue to alter stigmatizing attitudes towards people living with HIV/AIDS. In October 2009, the USA overturned a 22-year-old ban on HIV-infected visitors and immigrants (as part of the Ryan White HIV/AIDS Treatment Extension Act), which represents one example of policy-level changes that may ultimately reduce stigmatizing attitudes. In addition to structural changes, the field requires individual-level interventions to help individuals cope with HIV-related stigma. Insights gleaned from research on other stigmatized characteristics, including overweight/obesity [31], sexual orientation [32], mental illness [33], and race/ethnicity [34], may help clinicians promote adaptive coping in response to HIV-related stigma among MSM. In addition, recent research has begun to identify psychological mechanisms linking stigma-related stressors to health disparities in lesbian, gay, and bisexual populations [35]. This work highlights modifiable processes that can be targeted in the development of integrative HIV interventions that address the broader health concerns of MSM.
These results should be considered in light of the study’s limitations. First, although we used reliable and valid measures of HIV risk behavior and mental health variables [16, 17], these were self-reported data. The audio computer-assisted self-interview instruments provided greater anonymity, which likely reduced demand characteristics and therefore increased accuracy of self-report measures. Second, we did not use an established measure of HIV-related stigma, and our measure combined items assessing both injunctive and descriptive forms of stigma. Although there is no standardized measure of this construct across studies [4], measures are beginning to be validated [36, 37], which represents an important area for future study [38]. Third, although the prospective design is a methodological improvement over prior studies, we cannot rule out reverse causality (i.e., that mental health status leads to greater perceptions of stigma) [39]. Moreover, there is the potential for symptom overlap between the stigma items (fear and shame) and the mental health variables (anxiety and depression, respectively). However, shame was not included in the Patient Health Questionnaire items on depression, and the anxiety items assessed chronic worry and physiological sensations rather than fear-based symptoms, thereby reducing the likelihood of confounding. Fourth, the sample was restricted to an urban setting, which may not generalize to other populations of HIV-infected MSM. Finally, although our study documented statistical significance, there is currently no accepted convention for reporting effect size estimates within HLM. These results should therefore be interpreted with caution until their practical significance can be established. We note, however, that a recent meta-analysis of stigma and health among HIV-infected individuals documented medium effect sizes [4], demonstrating the practical significance of the experience of stigma for individuals living with HIV.
This study raises several important questions that warrant further examination. Given the lack of mediation in the current study, the identification of mechanisms that underlie the association between stigma and sexual risk behaviors represents an important area for future inquiry. Future research is also needed to understand how stigma influences mental health and health risk behaviors throughout the course of HIV disease progression. The experience of stigma may be especially pronounced for individuals who are recently infected and therefore have fewer resources to effectively cope with stigma. Indeed, secondary analyses indicated that HIV-infected individuals who were more recently diagnosed had significantly higher levels of perceived shame (but not fear). When we controlled for time since diagnosis in the models, the direction and magnitude of the results remained unchanged. However, given that our sample was largely comprised of men who had lived with the diagnosis for many years, we were likely underpowered to examine whether stigma was a stronger predictor of mental and behavioral health outcomes among recently diagnosed individuals. Finally, greater empirical attention should also be paid to identifying factors that may buffer MSM from the negative impact of stigma on health. For instance, future research would benefit from the inclusion of moderators at the individual (e.g., emotion regulation), family (e.g., social support), and community level (e.g., policies that protect sexual minorities).
There were several strengths to the current study that make it an important contribution to the literature on HIV stigma and health. We had a large, diverse sample of MSM participants who were recruited at the site of their primary care, which increases generalizability of the results across sociodemographic groups. In addition, we used a prospective design, increasing our ability to establish causal inferences. Finally, data from this study are among the first to document that perceived HIV-related stigma may lead to behaviors that increase risk for HIV transmission, which has important public health implications. Taken together, these results highlight the need for the development of prevention interventions that reduce stigma. Such interventions are warranted in order to improve the health and wellbeing of HIV-infected MSM, and to enhance the efficacy of existing interventions to reduce HIV transmission at a population level.
References
Herek GM., Capitanio JP, Widaman KF. HIV-related stigma and knowledge in the United States: Prevalence and trends, 1991–1999. Am J Public Health. 2002; 92:371–377.
Maman S, Abler L, Parker L, et al. A comparison of HIV stigma and discrimination in five international sites: The influence of care and treatment resources in high prevalence settings. Soc Sci Med. 2009; 68:2271–2278.
Ickovics J. HIV-related stigma and discrimination in Asia: A review of the human development consequences. United Nations Development Programme, New York; 2007.
Logie C, Gadalla TM. Meta-analysis of health and demographic correlates of stigma toward people living with HIV. AIDS Care. 2009; 21:742–753.
Centers for Disease Control and Prevention. HIV prevalence estimates—United States, 2006. MMWR. 2008; 57:1073–1076.
Dowshen N, Bonns HJ, Garofalo R. Experiences of HIV-related stigma among men who have sex with men. AIDS Patient Care STDS. 2009; 23:371–376.
Courtenay-Quirk C, Wolitski RJ, Parsons JT. Is HIV/AIDS stigma dividing the gay community? Perceptions of HIV-positive men who have sex with men. AIDS Educ Prev. 2006; 18:56–67.
Cloete A, Simbavi LC, Kalichman SC, Strebel A, Henda N. Stigma and discrimination experiences of HIV-positive men who have sex with men in Cape Town, South Africa. AIDS Care. 2008; 20:1105–1110.
Preston DB, D’Augelli AR, Kassab CD, Starks MT. The relationship of stigma to the sexual risk behavior of men who have sex with men. AIDS Educ Prev. 2007; 19:218–230.
Parsons JT, Halkitis PN, Wotlitski et al. Correlates of sexual risk behaviors among HIV-positive men who have sex with men. AIDS Educ Prev. 2003;15:383–400.
Knauz RO, Safren SA, O'Cleirigh C, et al. Developing an HIV-prevention intervention for HIV-infected men who have sex with men in HIV care: Project enhance. AIDS Behav. 2007; 11: S117-126.
Safren SA, O’Cleirigh C, Skeer M, et al (2011) Demonstration and evaluation of a peer-delivered, individually-tailored, HIV prevention intervention for HIV-infected MSM in their primary care setting. AIDS Behav (in press).
Mayer KH, Mimiaga MJ, VanDerwarker R, Goldhammer H, Bradford JB. Fenway Community Health’s model of integrated community-based LGBT care, education, and research. In: Meyer IH, Northridge ME, eds. The Health of Sexual Minorities. Springer, New York; 2007: 693–715.
Koester KA, Maiorana AE, Vernon K, Myers J, Dawson-Rose C, Morin S. Implementation of HIV prevention interventions with people living with HIV/AIDS in clinical settings: Challenges and lessons learned. AIDS Behav. 2007; 11: S17-S29.
Koblin BA, Chesney MA, Husnik MJ, et al. High-risk behaviors among men who have sex with men in 6 US cities: Baseline data from the EXPLORE study. Am J Public Health. 2003; 93:926–932.
Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999; 282:1737–1744.
Kroenke K, Spitzer RL, Williams JB. The PHQ-9: Validity of a brief depression severity measure. J Gen Intern Med. 2001; 16:606–613.
Raudenbush S, Bryk A, Cheong YF, Congdon R, du Toit M. HLM 6: Hierarchical Linear and Nonlinear Modeling. Lincolnwood, IL: Scientific Software International; 2004.
Sobel ME. Asymptotic confidence intervals for indirect effects in structural equation models. In S. Leinhart (Ed.), Sociological Methodology (pp. 290–312). San Francisco: Jossey-Bass; 1982.
Wight, RG. Precursive depression among HIV infected AIDS caregivers over time. Soc Sci Med. 2000; 51:759–770.
Berg CJ, Michelson SE, Safren SA. Behavioral aspects of HIV care: Adherence, depression, substance use, and HIV-transmission behaviors. Infect Dis Clin North Am. 2007; 21:181–200.
Mayer K, O’Cleirigh C, Skeer M, et al., Which HIV-infected MSM in care are engaging in risky sex and acquiring sexually transmitted infections: Findings from a Boston community health center. Sex Transm Infect. 2010; 86:66–70.
Hatzenbuehler ML, Nolen-Hoeksema S, Erickson SJ. Minority stress predictors of HIV risk behavior, substance use, and depressive symptoms: Results from a prospective study of bereaved gay men. Health Psychol. 2008; 27: 455–462.
Stall R, Mills TC, Williamston J, et al. Association of co-occurring psychosocial health problems and increased vulnerability to HIV/AIDS among urban men who have sex with men. Am J Public Health. 2003; 93:939–942.
Singer M. AIDS and the health crisis of the US urban poor: The perspective of critical medical anthropology. Soc Sci Med. 1994; 39:931–948.
Blascovich J, Mendes WB, Hunter S, Lickel B. (2000). Stigma, threat, and social interactions. In Heatherton TF, Kleck RE, Hebl MR, Hull JG, eds. The Social Psychology of Stigma. New York: Guilford Press; 2000: 307–333.
Pachankis JE. The psychological implications of concealing a stigma: A cognitive-affective-behavioral model. Psychol Bull. 2008; 133:328–345.
Kendler KS, Hettema JM, Butera F, Gardner CO, Prescott CA. Life event dimensions of loss, humiliation, entrapment, and danger in the prediction of onsets of major depression and generalized anxiety. Arch Gen Psychiatry. 2003; 60:789–796.
Sikkema KJ, Hansen NB, Meade CS, Kochman A, Fox AM. Psychosocial predictors of sexual HIV transmission risk behavior among HIV-positive adults with a sexual abuse history in childhood. Arch Sex Behav. 2009; 38:121–134.
Crepaz N, Marks G. Towards an understanding of sexual risk behavior in people living with HIV: A review of social, psychological, and medical findings. AIDS. 2002;16:135–149.
Myers A, Rosen JC. Obesity, stigmatization, and coping: Relation to mental health symptoms, body image, and self-esteem. Int J Obes Relat Metab Disord. 1999; 23:221–240.
Hatzenbuehler ML, Nolen-Hoeksema S, Dovidio JF. How does stigma “get under the skin?” The mediating role of emotion regulation. Psychol Sci. 2009; 20:1282–1289.
Hinshaw SP, Stier A. Stigma as related to mental disorders. Ann Rev Clin Psychol. 2008; 4:367–393.
Miller CT, Kaiser CR. A theoretical perspective on coping with stigma. J Soc Issues. 2001; 57:73–92.
Hatzenbuehler ML. How does sexual minority stigma “get under the skin?” A psychological mediation framework. Psychological Bulletin. 2009; 135:707–730.
Wright K, Naar-King S, Lam P, Templin T, Frey M. Stigma scale revised: Reliability and validity of a brief measure of stigma for HIV + youth. J Adolesc Health. 2007; 40: 96–98.
Bunn JY, Solomon SE, Miller C, Forehand R. Measurement of stigma in people with HIV: A reexamination of the HIV stigma scale. AIDS Educ Prev. 2007; 19:198–208.
Mak WS, Poon CYM, Pun LYK, Cheung SF. Meta-analysis of stigma and mental health. Soc Sci Med. 2007; 65:245–261.
Meyer IH. Prejudice as stress: Conceptual problems for measurement. Am J Public Health. 2003;93:262–265.
Acknowledgments
This study was supported by NIMH grant 5R01MH068746-05 and HRSA grant H97HA01293 awarded to Drs. Kenneth H. Mayer and Steven A. Safren.
Conflicts of Interest Statement
The authors have no conflicts of interest to report.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Hatzenbuehler, M.L., O’Cleirigh, C., Mayer, K.H. et al. Prospective Associations Between HIV-Related Stigma, Transmission Risk Behaviors, and Adverse Mental Health Outcomes in Men Who Have Sex with Men. ann. behav. med. 42, 227–234 (2011). https://doi.org/10.1007/s12160-011-9275-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12160-011-9275-z